Health Risks


Weight Problems Take a Hefty Toll on Body and Mind
In the old spiritual, “Dem Bones,” each body part is linked to the next one in line: the thigh bone to the knee bone, the knee bone to the leg bone, and so on. But one body “part”-weight-is connected to virtually all of the others. A healthy weight sets the stage for bones, muscles, brain, heart, and others to play their parts smoothly and efficiently for many years.
Excess weight, especially obesity, diminishes almost every aspect of health, from reproductive and respiratory function to memory and mood. Obesity increases the risk of several debilitating, and deadly diseases, including diabetes, heart disease, and some cancers. It does this through a variety of pathways, some as straightforward as the mechanical stress of carrying extra pounds and some involving complex changes in hormones and metabolism. Obesity decreases the quality and length of life, and increases individual, national, and global healthcare costs. The good news, though, is that weight loss can curtail some obesity-related risks. (1) Losing as little as 5 to 10 percent of body weight offers meaningful health benefits to people who are obese, even if they never achieve their “ideal” weight, and even if they only begin to lose weight later in life.
Entire books have been written detailing the effects of obesity on various measures of health. This article briefly summarizes associations between obesity and adult health.
Obesity and Diabetes
The condition most strongly influenced by body weight is type 2 diabetes. In the Nurses’ Health Study, which followed 114,000 middle-age women for 14 years, the risk of developing diabetes was 93 times higher among women who had a body mass index (BMI) of 35 or higher at the start of the study, compared with women with BMIs lower than 22. (2) Weight gain during adulthood also increased diabetes risk, even among women with BMIs in the healthy range. The Health Professionals Follow-Up Study found a similar association in men. (3)
More recently, investigators conducted a systematic review of 89 studies on weight-related diseases and then did a statistical summary, or meta-analysis, of the data. Of the 18 weight-related diseases they studied, diabetes was at the top of the risk list: Compared with men and women in the normal weight range (BMI lower than 25), men with BMIs of 30 or higher had a sevenfold higher risk of developing type 2 diabetes, and women with BMIs of 30 or higher had a 12-fold higher risk. (4)
Fat cells, especially those stored around the waist,secrete hormones and other substances that fire inflammation. Although inflammation is an essential component of the immune system and part of the healing process, inappropriate inflammation causes a variety of health problems. Inflammation can make the body less responsive to insulin and change the way the body metabolizes fats and carbohydrates, leading to higher blood sugar levels and, eventually, to diabetes and its many complications. (5) Several large trials have shown that moderate weight loss can prevent or delay the start of diabetes in people who are at high risk. (6-8)
Obesity and Cardiovascular Disease
Body weight is directly associated with various cardiovascular risk factors. As BMI increases, so do blood pressure, low-density lipoprotein (LDL, or “bad”) cholesterol, triglycerides, blood sugar, and inflammation. These changes translate into increased risk for coronary heart disease, stroke, and cardiovascular death:
- Obesity and Coronary Artery Disease. Numerous studies have demonstrated a direct association between excess body weight and coronary artery disease (CAD). The BMI-CAD Collaboration Investigators conducted a meta-analysis of 21 long-term studies that followed more than 300,000 participants for an average of 16 years. Study participants who were overweight had a 32 percent higher risk of developing CAD, compared with participants who were at a normal weight; those who were obese had an 81 percent higher risk. (9) Although adjustment for blood pressure and cholesterol levels slightly lowered the risk estimates, they remained highly significant for obesity. The investigators estimated that the effect of excess weight on blood pressure and blood cholesterol accounts for only about half of the obesity-related increased risk of coronary heart disease.
- Obesity and Stroke. Ischemic (clot-caused) stroke and coronary artery disease share many of the same disease processes and risk factors. A meta-analysis of 25 prospective cohort studies with 2.3 million participants demonstrated a direct, graded association between excess weight and stroke risk. Overweight increased the risk of ischemic stroke by 22 percent, and obesity increased it by 64 percent. There was no significant relationship between overweight or obesity and hemorrhagic (bleeding-caused) stroke, however. (10) A repeat analysis that statistically accounted for blood pressure, cholesterol, and diabetes weakened the associations, suggesting that these factors mediate the effect of obesity on stroke.
- Obesity and Cardiovascular Death. In a meta-analysis of 26 observational studies that included 390,000 men and women, several racial and ethnic groups, and samples from the U.S. and other countries, obesity was significantly associated with death from CAD and cardiovascular disease. Women with BMIs of 30 or higher had a 62 percent greater risk of dying early from CAD and also had a 53 percent higher risk of dying early from any type of cardiovascular disease, compared with women who had BMIs in the normal range (18.5 to 24.9). Men with BMIs of 30 or higher had similarly elevated risks. (11)
The good news is that weight loss of 5 to 10 percent of body weight can lower blood pressure, LDL cholesterol, and triglycerides, and improve other cardiovascular risk factors. (12-14)
Obesity and Cancer
The association between obesity and cancer is not quite as clear as that for diabetes and cardiovascular disease. This is due in part to the fact that cancer is not a single disease but a collection of individual diseases.

Obesity, Depression, and Quality of Life
The high rates of obesity and depression, and their individual links with cardiovascular disease, have prompted many investigators to explore the relationship between weight and mood. An analysis of 17 cross-sectional studies found that people who were obese were more likely to have depression than people with healthy weights. (17) Since the studies included in the analysis assessed weight and mood only at one point in time, the investigators could not say whether obesity increases the risk of depression or depression increases the risk of obesity. New evidence confirms that the relationship between obesity and depression may be a two-way street: A meta-analysis of 15 long-term studies that followed 58,000 participants for up to 28 years found that people who were obese at the start of the study had a 55 percent higher risk of developing depression by the end of the follow-up period, and people who had depression at the start of the study had a 58 percent higher risk of becoming obese. (18)
Although a biological link between obesity and depression has not yet been definitively identified, possible mechanisms include activation of inflammation, changes in the hypothalamic-pituitary-adrenal axis, insulin resistance, and social or cultural factors.
Studies of the effect of obesity on specific health outcomes such as diabetes or depression provide only a glimpse of the full impact of obesity on health and well-being. Health-related quality of life (HRQoL) integrates the effect of obesity (or any other condition) across physical, psychological, and social functioning. Although HRQoL is a relatively young field of research, a number of studies have evaluated the overall impact of obesity on HRQoL. Among 31 studies in adults, the majority demonstrated that obesity was significantly associated with reduced HRQoL, compared with normal weight. (19) Researchers found a similar association among five HRQoL studies in children and adolescents.
Obesity and Reproduction
Obesity can influence various aspects of reproduction, from sexual activity to conception. Among women, the association between obesity and infertility, primarily ovulatory infertility, is represented by a classic U-shaped curve. In the Nurses’ Health Study, infertility was lowest in women with BMIs between 20 and 24, and increased with lower and higher BMIs. (20) This study suggests that 25 percent of ovulatory infertility in the United States may be attributable to obesity. During pregnancy, obesity increases the risk of early and late miscarriage, gestational diabetes, preeclampsia, and complications during labor and delivery. (21) It also slightly increases the chances of bearing a child with congenital anomalies. (22) One small randomized trial suggests that modest weight loss improves fertility in obese women. (23)

Sexual function may also be affected by obesity. Data from the Health Professionals Follow-Up Study, (26) the National Health and Nutrition Examination Survey (NHANES), (27) and the Massachusetts Male Aging Study (28) indicate that the odds of developing erectile dysfunction increase with increasing BMI. Of note, weight loss appears to be mildly helpful in maintaining erectile function. (29) The effect of obesity on female sexual function is less clear. In a recent French study, obese women were less likely than normal-weight women to report having had a sexual partner in the preceding 12 months, but the prevalence of sexual dysfunction was similar in both groups. (30) In a smaller survey of 118 women, Esposito and colleagues found that obese women had lower scores on the Female Sexual Function Index, with strong correlations between increasing BMI and problems with arousal, lubrication, orgasm, and satisfaction. (31)
Obesity and Lung Function/Respiratory Disease
Excess weight impairs respiratory function via mechanical and metabolic pathways. The accumulation of abdominal fat, for example, may limit the descent of the diaphragm, and in turn, lung expansion, while the accumulation of visceral fat can reduce the flexibility of the chest wall, sap respiratory muscle strength, and narrow airways in the lungs. (32) Cytokines generated by the low-grade inflammatory state that accompanies obesity may also impede lung function.
Asthma and obstructive sleep apnea are two common respiratory diseases that have been linked with obesity. In a meta-analysis of seven prospective studies that included 333,000 subjects, obesity increased the risk of developing asthma in both men and women by 50 percent. (33) Obesity is also a major contributor to obstructive sleep apnea (OSA), which is estimated to affect approximately one in five adults; one in 15 adults has moderate or severe obstructive sleep apnea. This condition is associated with daytime sleepiness, accidents, hypertension, cardiovascular disease, and premature mortality. Between 50 percent and 75 percent of individuals with OSA are obese. (32) Clinical trials suggest that modest weight loss can be helpful when treating sleep apnea. (34, 35)
Obesity, Memory, and Cognitive Function
Alzheimer’s disease and dementia are scourges of populations that enjoy a long life span. In the United States, these diseases affect more than 7.5 million people, most of them over age 65. At 65, the estimated lifetime risk for Alzheimer’s disease is 17.2 percent in women and 9.1 percent in men. (36) Body weight is a potentially modifiable risk factor for Alzheimer’s disease and dementia. A meta-analysis of 10 prospective cohort studies that included almost 42,000 subjects followed for three to 36 years demonstrated a U-shaped association between BMI and Alzheimer’s disease. Compared with being in the normal weight range, being underweight was associated with a 36 percent higher risk of Alzheimer’s disease while being obese was associated with a 42 percent higher risk. (37) The associations were stronger in studies with longer follow-up. A more recent meta-analysis demonstrated a similarly strong association between obesity and Alzheimer’s disease. (38)
Obesity and Musculoskeletal Disorders
Excess weight places mechanical and metabolic strains on bones, muscles, and joints. In the United States, an estimated 46 million adults (about one in five) report doctor-diagnosed arthritis. (1) Osteoarthritis of the knee and hip are both positively associated with obesity, and obese patients account for one-third of all joint replacement operations. (39) Obesity also increases the risk of back pain, lower limb pain, and disability due to musculoskeletal conditions.
Obesity and Other Conditions
A number of additional health outcomes have been linked to excess weight. These include the development of gallstones in men (40) and women, (41) as well as gout, (42, 43) chronic kidney disease, (44) and nonalcoholic fatty liver disease. (25,45)
Obesity and Mortality
Given the adverse consequences of obesity on multiple aspects of health, it makes sense that the condition also shortens survival or increases premature mortality. However, pinning down the contribution of obesity to premature mortality has been fraught with methodological problems and controversy.
Two of the biggest problems that researchers must cope with are reverse causation-low body weight is often the result of chronic disease, rather than being a cause of it-and the effect of smoking. People with BMIs below 25 are a mix of healthy individuals and those who have lost weight due to cancer or some other disease that may or may not have been diagnosed. Smoking also confuses the issue because smokers tend to weigh less than their nonsmoking counterparts. When reverse causation and the adverse effects of smoking aren’t fully accounted for, death rates among lean individuals will be inflated and those among overweight and obese individuals will be diminished. That was a problem with a widely reported study based on data from NHANES, which estimated relatively low numbers of excess obesity-related deaths. (46) A careful critique of using the NHANES data to estimate mortality demonstrated that correcting for statistical biases significantly increased the estimate of excess deaths attributable to obesity. (47)
Findings from larger studies that have more accurately accounted for reverse causation and smoking clearly show that increasing weight increases the risks of dying from cardiovascular disease, cancer, and other causes. In a 14-year study of a million-person cohort, researchers restricted their analyses to initially healthy nonsmokers. The risk of death from all causes, cardiovascular disease, cancer, or other diseases increased as BMI increased above the healthiest range of 23.5 to 24.9 in men and 22.0 to 23.4 in women. (48) A similar association between weight and mortality was observed in another carefully controlled analysis of five prospective cohort studies (49) and a prospective study of more than 500,000 older men and women in the National Institutes of Health/AARP study. (50)
The Bottom Line
Obesity harms virtually every aspect of health, from shortening life and contributing to chronic conditions such as diabetes and cardiovascular disease to interfering with sexual function, breathing, mood, and social interactions. Obesity isn’t necessarily a permanent condition. Diet, exercise, medications and even surgery can lead to weight loss. Yet it is much much harder to lose weight than it is to gain it. Prevention of obesity, beginning at an early age and extending across a lifespan could vastly improve individual and public health, reduce suffering, and save billions of dollars each year in health care costs.
- National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults . 2002. Accessed January 25, 2012.
- Colditz GA, Willett WC, Rotnitzky A, Manson JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med . 1995; 122:4816.
- Koh-Banerjee P, Wang Y, Hu FB, Spiegelman D, Willett WC, Rimm EB. Changes in body weight and body fat distribution as risk factors for clinical diabetes in US men. Am J Epidemiol . 2004; 159:11509.
- Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health . 2009; 9:88.
- Rocha VZ, Libby P. Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol . 2009; 6:399409.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med . 2002; 346:393403.
- Li G, Zhang P, Wang J, et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study. Lancet . 2008; 371:17839.
- Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med . 2001; 344:134350.
- Bogers RP, Bemelmans WJ, Hoogenveen RT, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300,000 persons. Arch Intern Med . 2007; 167:17208.
- Strazzullo P, DElia L, Cairella G, Garbagnati F, Cappuccio FP, Scalfi L. Excess body weight and incidence of stroke: meta-analysis of prospective studies with 2 million participants. Stroke . 2010; 41:e41826.
- McGee DL. Body mass index and mortality: a meta-analysis based on person-level data from twenty-six observational studies. Ann Epidemiol . 2005; 15:8797.
- Wing RR. Long-term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes mellitus: four-year results of the Look AHEAD trial. Arch Intern Med . 2010; 170:156675.
- Dengo AL, Dennis EA, Orr JS, et al. Arterial destiffening with weight loss in overweight and obese middle-aged and older adults. Hypertension . 2010; 55:85561.
- de las Fuentes L, Waggoner AD, Mohammed BS, et al. Effect of moderate diet-induced weight loss and weight regain on cardiovascular structure and function. J Am Coll Cardiol . 2009; 54:237681.
- American Institute for Cancer Research, World Cancer Research Fund. Food, nutrition, physical activity and the prevention of cancer. Washington, D.C.: American Institute for Cancer Research ; 2007.
- Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE. Adult weight change and risk of postmenopausal breast cancer. JAMA . 2006; 296:193201.
- de Wit L, Luppino F, van Straten A, Penninx B, Zitman F, Cuijpers P. Depression and obesity: a meta-analysis of community-based studies. Psychiatry Res . 2010; 178:2305.
- Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry . 2010; 67:2209.
- Kim D, Kawachi I. Obesity and health-related quality of life. In: Hu FB, ed. Obesity Epidemiology. London: Oxford University Press; 2008:23460.
- Rich-Edwards JW, Spiegelman D, Garland M, et al. Physical activity, body mass index, and ovulatory disorder infertility. Epidemiology . 2002; 13:18490.
- Huda SS, Brodie LE, Sattar N. Obesity in pregnancy: prevalence and metabolic consequences. Semin Fetal Neonatal Med . 2010; 15:706.
- Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. JAMA . 2009; 301:63650.
- Clark AM, Ledger W, Galletly C, et al. Weight loss results in significant improvement in pregnancy and ovulation rates in anovulatory obese women. Hum Reprod . 1995; 10:270512.
- Hammoud AO, Wilde N, Gibson M, Parks A, Carrell DT, Meikle AW. Male obesity and alteration in sperm parameters. Fertil Steril . 2008; 90:22225.
- Chavarro JE, Toth TL, Wright DL, Meeker JD, Hauser R. Body mass index in relation to semen quality, sperm DNA integrity, and serum reproductive hormone levels among men attending an infertility clinic. Fertil Steril . 2010; 93:222231.
- Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Glasser DB, Rimm EB. A prospective study of risk factors for erectile dysfunction. J Urol . 2006; 176:21721.
- Saigal CS, Wessells H, Pace J, Schonlau M, Wilt TJ. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med . 2006; 166:20712.
- Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol . 2000; 163:4603.
- Wing RR, Rosen RC, Fava JL, et al. Effects of weight loss intervention on erectile function in older men with type 2 diabetes in the Look AHEAD trial. J Sex Med . 2010; 7:15665.
- Bajos N, Wellings K, Laborde C, Moreau C. Sexuality and obesity, a gender perspective: results from French national random probability survey of sexual behaviours. BMJ . 2010; 340:c2573.
- Esposito K, Ciotola M, Giugliano F, et al. Association of body weight with sexual function in women. Int J Impot Res . 2007; 19:353-7.
- McClean KM, Kee F, Young IS, Elborn JS. Obesity and the lung: 1. Epidemiology. Thorax . 2008; 63:64954.
- Beuther DA, Sutherland ER. Overweight, obesity, and incident asthma: a meta-analysis of prospective epidemiologic studies. Am J Respir Crit Care Med . 2007; 175:6616.
- Nerfeldt P, Nilsson BY, Mayor L, Udden J, Friberg D. A two-year weight reduction program in obese sleep apnea patients. J Clin Sleep Med . 2010; 6:47986.
- Tuomilehto HP, Seppa JM, Partinen MM, et al. Lifestyle intervention with weight reduction: first-line treatment in mild obstructive sleep apnea. Am J Respir Crit Care Med . 2009; 179:3207.
- Alzheimers Association. Alzheimers Facts and Figures. Alzheimers & Dementia . 2010; 6. Accessed January 25, 2012.
- Beydoun MA, Beydoun HA, Wang Y. Obesity and central obesity as risk factors for incident dementia and its subtypes: a systematic review and meta-analysis. Obes Rev . 2008; 9:204-18
- Profenno LA, Porsteinsson AP, Faraone SV. Meta-analysis of Alzheimers disease risk with obesity, diabetes, and related disorders. Biol Psychiatry . 2010; 67:50512.
- Anandacoomarasamy A, Caterson I, Sambrook P, Fransen M, March L. The impact of obesity on the musculoskeletal system. Int J Obes (Lond) . 2008; 32:21122.
- Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. Prospective study of abdominal adiposity and gallstone disease in US men. Am J Clin Nutr . 2004; 80:3844.
- Stampfer MJ, Maclure KM, Colditz GA, Manson JE, Willett WC. Risk of symptomatic gallstones in women with severe obesity. Am J Clin Nutr . 1992; 55:6528.
- Bhole V, de Vera M, Rahman MM, Krishnan E, Choi H. Epidemiology of gout in women: Fifty-two-year followup of a prospective cohort. Arthritis Rheum . 2010; 62:106976.
- Choi HK, Atkinson K, Karlson EW, Curhan G. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: the Health Professionals Follow-up Study. Arch Intern Med . 2005; 165:7428.
- Kopple JD. Obesity and chronic kidney disease. J Ren Nutr . 2010; 20:S2930.
- Tsuneto A, Hida A, Sera N, et al. Fatty liver incidence and predictive variables. Hypertens Res . 2010; 33:63843.
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Cause-specific excess deaths associated with underweight, overweight, and obesity. JAMA . 2007; 298:202837.
- Greenberg JA. Correcting biases in estimates of mortality attributable to obesity. Obesity (Silver Spring) . 2006; 14:20719.
- Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW, Jr. Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med . 1999; 341:1097105.
- Allison DB, Fontaine KR, Manson JE, Stevens J, VanItallie TB. Annual deaths attributable to obesity in the United States. JAMA . 1999; 282:15308.
- Adams KF, Schatzkin A, Harris TB, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med . 2006; 355:76378.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Published: 27 February 2019
Obesity: global epidemiology and pathogenesis
- Matthias Blüher 1
Nature Reviews Endocrinology volume 15 , pages 288–298 ( 2019 ) Cite this article
55k Accesses
2456 Citations
988 Altmetric
Metrics details
- Epidemiology
- Health policy
- Pathogenesis
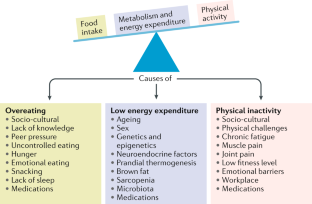
The prevalence of obesity has increased worldwide in the past ~50 years, reaching pandemic levels. Obesity represents a major health challenge because it substantially increases the risk of diseases such as type 2 diabetes mellitus, fatty liver disease, hypertension, myocardial infarction, stroke, dementia, osteoarthritis, obstructive sleep apnoea and several cancers, thereby contributing to a decline in both quality of life and life expectancy. Obesity is also associated with unemployment, social disadvantages and reduced socio-economic productivity, thus increasingly creating an economic burden. Thus far, obesity prevention and treatment strategies — both at the individual and population level — have not been successful in the long term. Lifestyle and behavioural interventions aimed at reducing calorie intake and increasing energy expenditure have limited effectiveness because complex and persistent hormonal, metabolic and neurochemical adaptations defend against weight loss and promote weight regain. Reducing the obesity burden requires approaches that combine individual interventions with changes in the environment and society. Therefore, a better understanding of the remarkable regional differences in obesity prevalence and trends might help to identify societal causes of obesity and provide guidance on which are the most promising intervention strategies.
Obesity prevalence has increased in pandemic dimensions over the past 50 years.
Obesity is a disease that can cause premature disability and death by increasing the risk of cardiometabolic diseases, osteoarthritis, dementia, depression and some types of cancers.
Obesity prevention and treatments frequently fail in the long term (for example, behavioural interventions aiming at reducing energy intake and increasing energy expenditure) or are not available or suitable (bariatric surgery) for the majority of people affected.
Although obesity prevalence increased in every single country in the world, regional differences exist in both obesity prevalence and trends; understanding the drivers of these regional differences might help to provide guidance for the most promising intervention strategies.
Changes in the global food system together with increased sedentary behaviour seem to be the main drivers of the obesity pandemic.
The major challenge is to translate our knowledge of the main causes of increased obesity prevalence into effective actions; such actions might include policy changes that facilitate individual choices for foods that have reduced fat, sugar and salt content.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
195,33 € per year
only 16,28 € per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Obesity and the risk of cardiometabolic diseases
Pedro L. Valenzuela, Pedro Carrera-Bastos, … Alejandro Lucia

Obesity-induced and weight-loss-induced physiological factors affecting weight regain
Marleen A. van Baak & Edwin C. M. Mariman

The genetics of obesity: from discovery to biology
Ruth J. F. Loos & Giles S. H. Yeo
World Health Organization. Noncommunicable diseases progress monitor, 2017. WHO https://www.who.int/nmh/publications/ncd-progress-monitor-2017/en/ (2017).
Fontaine, K. R., Redden, D. T., Wang, C., Westfall, A. O. & Allison, D. B. Years of life lost due to obesity. JAMA 289 , 187–193 (2003).
PubMed Google Scholar
Berrington de Gonzalez, A. et al. Body-mass index and mortality among 1.46 million white adults. N. Engl. J. Med. 363 , 2211–2219 (2010).
CAS PubMed Google Scholar
Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900000 adults: collaborative analyses of 57 prospective studies. Lancet 373 , 1083–1096 (2009).
PubMed Central Google Scholar
Woolf, A. D. & Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 81 , 646–656 (2003).
PubMed PubMed Central Google Scholar
Bray, G. A. et al. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 18 , 715–723 (2017).
World Health Organization. Obesity and overweight. WHO https://www.who.int/mediacentre/factsheets/fs311/en/ (2016).
World Health Organization. Political declaration of the high-level meeting of the general assembly on the prevention and control of non-communicable diseases. WHO https://www.who.int/nmh/events/un_ncd_summit2011/political_declaration_en.pdf (2012).
Franco, M. et al. Population-wide weight loss and regain in relation to diabetes burden and cardiovascular mortality in Cuba 1980-2010: repeated cross sectional surveys and ecological comparison of secular trends. BMJ 346 , f1515 (2013).
Swinburn, B. A. et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet 378 , 804–814 (2011).
Yanovski, J. A. Obesity: Trends in underweight and obesity — scale of the problem. Nat. Rev. Endocrinol. 14 , 5–6 (2018).
Heymsfield, S. B. & Wadden, T. A. Mechanisms, pathophysiology, and management of obesity. N. Engl. J. Med. 376 , 254–266 (2017).
Murray, S., Tulloch, A., Gold, M. S. & Avena, N. M. Hormonal and neural mechanisms of food reward, eating behaviour and obesity. Nat. Rev. Endocrinol. 10 , 540–552 (2014).
Farooqi, I. S. Defining the neural basis of appetite and obesity: from genes to behaviour. Clin. Med. 14 , 286–289 (2014).
Google Scholar
Anand, B. K. & Brobeck, J. R. Hypothalamic control of food intake in rats and cats. Yale J. Biol. Med. 24 , 123–140 (1951).
CAS PubMed PubMed Central Google Scholar
Zhang, Y. et al. Positional cloning of the mouse obese gene and its human homologue. Nature 372 , 425–432 (1994).
Coleman, D. L. & Hummel, K. P. Effects of parabiosis of normal with genetically diabetic mice. Am. J. Physiol. 217 , 1298–1304 (1969).
Farooqi, I. S. & O’Rahilly, S. 20 years of leptin: human disorders of leptin action. J. Endocrinol. 223 , T63–T70 (2014).
Börjeson, M. The aetiology of obesity in children. A study of 101 twin pairs. Acta Paediatr. Scand. 65 , 279–287 (1976).
Stunkard, A. J., Harris, J. R., Pedersen, N. L. & McClearn, G. E. The body-mass index of twins who have been reared apart. N. Engl. J. Med. 322 , 1483–1487 (1990).
Montague, C. T. et al. Congenital leptin deficiency is associated with severe early-onset obesity in humans. Nature 387 , 903–908 (1997).
Farooqi, I. S. et al. Effects of recombinant leptin therapy in a child with congenital leptin deficiency. N. Engl. J. Med. 341 , 879–884 (1999).
Clément, K. et al. A mutation in the human leptin receptor gene causes obesity and pituitary dysfunction. Nature 392 , 398–401 (1998).
Farooqi, I. S. et al. Dominant and recessive inheritance of morbid obesity associated with melanocortin 4 receptor deficiency. J. Clin. Invest. 106 , 271–279 (2000).
Krude, H. et al. Severe early-onset obesity, adrenal insufficiency and red hair pigmentation caused by POMC mutations in humans. Nat. Genet. 19 , 155–157 (1998).
Hebebrand, J., Volckmar, A. L., Knoll, N. & Hinney, A. Chipping away the ‘missing heritability’: GIANT steps forward in the molecular elucidation of obesity - but still lots to go. Obes. Facts 3 , 294–303 (2010).
Speliotes, E. K. et al. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat. Genet. 42 , 937–948 (2010).
Sharma, A. M. & Padwal, R. Obesity is a sign - over-eating is a symptom: an aetiological framework for the assessment and management of obesity. Obes. Rev. 11 , 362–370 (2010).
Berthoud, H. R., Münzberg, H. & Morrison, C. D. Blaming the brain for obesity: integration of hedonic and homeostatic mechanisms. Gastroenterology 152 , 1728–1738 (2017).
Government Office for Science. Foresight. Tackling obesities: future choices – project report. GOV.UK https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/287937/07-1184x-tackling-obesities-future-choices-report.pdf (2007).
World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th revision. WHO http://apps.who.int/classifications/icd10/browse/2010/en (2010).
Hebebrand, J. et al. A proposal of the European Association for the Study of Obesity to improve the ICD-11 diagnostic criteria for obesity based on the three dimensions. Obes. Facts 10 , 284–307 (2017).
Ramos Salas, X. et al. Addressing weight bias and discrimination: moving beyond raising awareness to creating change. Obes. Rev. 18 , 1323–1335 (2017).
Sharma, A. M. et al. Conceptualizing obesity as a chronic disease: an interview with Dr. Arya Sharma. Adapt. Phys. Activ Q. 35 , 285–292 (2018).
Hebebrand, J. et al. “Eating addiction”, rather than “food addiction”, better captures addictive-like eating behavior. Neurosci. Biobehav. Rev. 47 , 295–306 (2014).
Phelan, S. M. et al. Impact of weight bias and stigma on quality of care and outcomes for patients with obesity. Obes. Rev. 16 , 319–326 (2015).
Kushner, R. F. et al. Obesity coverage on medical licensing examinations in the United States. What is being tested? Teach Learn. Med. 29 , 123–128 (2017).
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 390 , 2627–2642 (2017).
NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 387 , 1377–1396 (2016).
Organisation for Economic Co-operation and Development. Obesity update 2017. OECD https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (2017).
Geserick, M. et al. BMI acceleration in early childhood and risk of sustained obesity. N. Engl. J. Med. 379 , 1303–1312 (2018).
Ezzati, M. & Riboli, E. Behavioral and dietary risk factors for noncommunicable diseases. N. Engl. J. Med. 369 , 954–964 (2013).
Kleinert, S. & Horton, R. Rethinking and reframing obesity. Lancet 385 , 2326–2328 (2015).
Roberto, C. A. et al. Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking. Lancet 385 , 2400–2409 (2015).
Lundborg, P., Nystedt, P. & Lindgren, B. Getting ready for the marriage market? The association between divorce risks and investments in attractive body mass among married Europeans. J. Biosoc. Sci. 39 , 531–544 (2007).
McCabe, M. P. et al. Socio-cultural agents and their impact on body image and body change strategies among adolescents in Fiji, Tonga, Tongans in New Zealand and Australia. Obes. Rev. 12 , 61–67 (2011).
Hayashi, F., Takimoto, H., Yoshita, K. & Yoshiike, N. Perceived body size and desire for thinness of young Japanese women: a population-based survey. Br. J. Nutr. 96 , 1154–1162 (2006).
Hardin, J., McLennan, A. K. & Brewis, A. Body size, body norms and some unintended consequences of obesity intervention in the Pacific islands. Ann. Hum. Biol. 45 , 285–294 (2018).
Monteiro, C. A., Conde, W. L. & Popkin, B. M. Income-specific trends in obesity in Brazil: 1975–2003. Am. J. Public Health 97 , 1808–1812 (2007).
Mariapun, J., Ng, C. W. & Hairi, N. N. The gradual shift of overweight, obesity, and abdominal obesity towards the poor in a multi-ethnic developing country: findings from the Malaysian National Health and Morbidity Surveys. J. Epidemiol. 28 , 279–286 (2018).
Gebrie, A., Alebel, A., Zegeye, A., Tesfaye, B. & Ferede, A. Prevalence and associated factors of overweight/ obesity among children and adolescents in Ethiopia: a systematic review and meta-analysis. BMC Obes. 5 , 19 (2018).
Rokholm, B., Baker, J. L. & Sørensen, T. I. The levelling off of the obesity epidemic since the year 1999 — a review of evidence and perspectives. Obes. Rev. 11 , 835–846 (2010).
Hauner, H. et al. Overweight, obesity and high waist circumference: regional differences in prevalence in primary medical care. Dtsch. Arztebl. Int. 105 , 827–833 (2008).
Myers, C. A. et al. Regional disparities in obesity prevalence in the United States: a spatial regime analysis. Obesity 23 , 481–487 (2015).
Wilkinson, R. G. & Pickett, K. The Spirit Level: Why More Equal Societies Almost Always Do Better 89–102 (Bloomsbury Press London, 2009).
Sarget, M. Why inequality is fatal. Nature 458 , 1109–1110 (2009).
Plachta-Danielzik, S. et al. Determinants of the prevalence and incidence of overweight in children and adolescents. Public Health Nutr. 13 , 1870–1881 (2010).
Bell, A. C., Ge, K. & Popkin, B. M. The road to obesity or the path to prevention: motorized transportation and obesity in China. Obes. Res. 10 , 277–283 (2002).
Ludwig, J. et al. Neighborhoods, obesity, and diabetes — a randomized social experiment. N. Engl. J. Med. 365 , 1509–1519 (2011).
Beyerlein, A., Kusian, D., Ziegler, A. G., Schaffrath-Rosario, A. & von Kries, R. Classification tree analyses reveal limited potential for early targeted prevention against childhood overweight. Obesity 22 , 512–517 (2014).
Reilly, J. J. et al. Early life risk factors for obesity in childhood: cohort study. BMJ 330 , 1357 (2005).
Kopelman, P. G. Obesity as a medical problem. Nature 404 , 635–643 (2000).
CAS Google Scholar
Bouchard, C. et al. The response to long-term overfeeding in identical twins. N. Engl. J. Med. 322 , 1477–1482 (1990).
Sadeghirad, B., Duhaney, T., Motaghipisheh, S., Campbell, N. R. & Johnston, B. C. Influence of unhealthy food and beverage marketing on children’s dietary intake and preference: a systematic review and meta-analysis of randomized trials. Obes. Rev. 17 , 945–959 (2016).
Gilbert-Diamond, D. et al. Television food advertisement exposure and FTO rs9939609 genotype in relation to excess consumption in children. Int. J. Obes. 41 , 23–29 (2017).
Frayling, T. M. et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 316 , 889–894 (2007).
Loos, R. J. F. & Yeo, G. S. H. The bigger picture of FTO-the first GWAS-identified obesity gene. Nat. Rev. Endocrinol. 10 , 51–61 (2014).
Wardle, J. et al. Obesity associated genetic variation in FTO is associated with diminished satiety. J. Clin. Endocrinol. Metab. 93 , 3640–3643 (2008).
Tanofsky-Kraff, M. et al. The FTO gene rs9939609 obesity-risk allele and loss of control over eating. Am. J. Clin. Nutr. 90 , 1483–1488 (2009).
Hess, M. E. et al. The fat mass and obesity associated gene (Fto) regulates activity of the dopaminergic midbrain circuitry. Nat. Neurosci. 16 , 1042–1048 (2013).
Fredriksson, R. et al. The obesity gene, FTO, is of ancient origin, up-regulated during food deprivation and expressed in neurons of feeding-related nuclei of the brain. Endocrinology 149 , 2062–2071 (2008).
Cohen, D. A. Neurophysiological pathways to obesity: below awareness and beyond individual control. Diabetes 57 , 1768–1773 (2008).
Richard, D. Cognitive and autonomic determinants of energy homeostasis in obesity. Nat. Rev. Endocrinol. 11 , 489–501 (2015).
Clemmensen, C. et al. Gut-brain cross-talk in metabolic control. Cell 168 , 758–774 (2017).
Timper, K. & Brüning, J. C. Hypothalamic circuits regulating appetite and energy homeostasis: pathways to obesity. Dis. Model. Mech. 10 , 679–689 (2017).
Kim, K. S., Seeley, R. J. & Sandoval, D. A. Signalling from the periphery to the brain that regulates energy homeostasis. Nat. Rev. Neurosci. 19 , 185–196 (2018).
Cutler, D. M., Glaeser, E. L. & Shapiro, J. M. Why have Americans become more obese? J. Econ. Perspect. 17 , 93–118 (2003).
Löffler, A. et al. Effects of psychological eating behaviour domains on the association between socio-economic status and BMI. Public Health Nutr. 20 , 2706–2712 (2017).
Chan, R. S. & Woo, J. Prevention of overweight and obesity: how effective is the current public health approach. Int. J. Environ. Res. Public Health 7 , 765–783 (2010).
Hsueh, W. C. et al. Analysis of type 2 diabetes and obesity genetic variants in Mexican Pima Indians: marked allelic differentiation among Amerindians at HLA. Ann. Hum. Genet. 82 , 287–299 (2018).
Schulz, L. O. et al. Effects of traditional and western environments on prevalence of type 2 diabetes in Pima Indians in Mexico and the US. Diabetes Care 29 , 1866–1871 (2006).
Rotimi, C. N. et al. Distribution of anthropometric variables and the prevalence of obesity in populations of west African origin: the International Collaborative Study on Hypertension in Blacks (ICSHIB). Obes. Res. 3 , 95–105 (1995).
Durazo-Arvizu, R. A. et al. Rapid increases in obesity in Jamaica, compared to Nigeria and the United States. BMC Public Health 8 , 133 (2008).
Hu, F. B., Li, T. Y., Colditz, G. A., Willett, W. C. & Manson, J. E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 289 , 1785–1791 (2003).
Rissanen, A. M., Heliövaara, M., Knekt, P., Reunanen, A. & Aromaa, A. Determinants of weight gain and overweight in adult Finns. Eur. J. Clin. Nutr. 45 , 419–430 (1991).
Zimmet, P. Z., Arblaster, M. & Thoma, K. The effect of westernization on native populations. Studies on a Micronesian community with a high diabetes prevalence. Aust. NZ J. Med. 8 , 141–146 (1978).
Ulijaszek, S. J. Increasing body size among adult Cook Islanders between 1966 and 1996. Ann. Hum. Biol. 28 , 363–373 (2001).
Snowdon, W. & Thow, A. M. Trade policy and obesity prevention: challenges and innovation in the Pacific Islands. Obes. Rev. 14 , 150–158 (2013).
McLennan, A. K. & Ulijaszek, S. J. Obesity emergence in the Pacific islands: why understanding colonial history and social change is important. Public Health Nutr. 18 , 1499–1505 (2015).
Becker, A. E., Gilman, S. E. & Burwell, R. A. Changes in prevalence of overweight and in body image among Fijian women between 1989 and 1998. Obes. Res. 13 , 110–117 (2005).
Swinburn, B., Sacks, G. & Ravussin, E. Increased food energy supply is more than sufficient to explain the US epidemic of obesity. Am. J. Clin. Nutr. 90 , 1453–1456 (2009).
Swinburn, B. A. et al. Estimating the changes in energy flux that characterize the rise in obesity prevalence. Am. J. Clin. Nutr. 89 , 1723–1728 (2009).
US Department of Agriculture. Food availability (per capita) data system. USDA https://www.ers.usda.gov/data-products/food-availability-per-capita-data-system/ (updated 29 Oct 2018).
Carden, T. J. & Carr, T. P. Food availability of glucose and fat, but not fructose, increased in the U.S. between 1970 and 2009: analysis of the USDA food availability data system. Nutr. J. 12 , 130 (2013).
Hall, K. D., Guo, J., Dore, M. & Chow, C. C. The progressive increase of food waste in America and its environmental impact. PLOS ONE 4 , e7940 (2009).
Scarborough, P. et al. Increased energy intake entirely accounts for increase in body weight in women but not in men in the UK between 1986 and 2000. Br. J. Nutr. 105 , 1399–1404 (2011).
McGinnis, J. M. & Nestle, M. The Surgeon General’s report on nutrition and health: policy implications and implementation strategies. Am. J. Clin. Nutr. 49 , 23–28 (1989).
Krebs-Smith, S. M., Reedy, J. & Bosire, C. Healthfulness of the U.S. food supply: little improvement despite decades of dietary guidance. Am. J. Prev. Med. 38 , 472–477 (2010).
Malik, V. S., Popkin, B. M., Bray, G. A., Després, J. P. & Hu, F. B. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 121 , 1356–1364 (2010).
Schulze, M. B. et al. Sugar-sweetened beverages, weight gain, and incidence of type 2 diabetes in young and middle-aged women. JAMA 292 , 927–934 (2004).
Mozaffarian, D., Hao, T., Rimm, E. B., Willett, W. C. & Hu, F. B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 364 , 2392–2404 (2011).
Malik, V. S. & Hu, F. B. Sugar-sweetened beverages and health: where does the evidence stand? Am. J. Clin. Nutr. 94 , 1161–1162 (2011).
Qi, Q. et al. Sugar-sweetened beverages and genetic risk of obesity. N. Engl. J. Med. 367 , 1387–1396 (2012).
Heiker, J. T. et al. Identification of genetic loci associated with different responses to high-fat diet-induced obesity in C57BL/6N and C57BL/6J substrains. Physiol. Genomics 46 , 377–384 (2014).
Wahlqvist, M. L. et al. Early-life influences on obesity: from preconception to adolescence. Ann. NY Acad. Sci. 1347 , 1–28 (2015).
Rohde, K. et al. Genetics and epigenetics in obesity. Metabolism . https://doi.org/10.1016/j.metabol.2018.10.007 (2018).
Article PubMed Google Scholar
Panzeri, I. & Pospisilik, J. A. Epigenetic control of variation and stochasticity in metabolic disease. Mol. Metab. 14 , 26–38 (2018).
Ruiz-Hernandez, A. et al. Environmental chemicals and DNA methylation in adults: a systematic review of the epidemiologic evidence. Clin. Epigenet. 7 , 55 (2015).
Quarta, C., Schneider, R. & Tschöp, M. H. Epigenetic ON/OFF switches for obesity. Cell 164 , 341–342 (2016).
Dalgaard, K. et al. Trim28 haploinsufficiency triggers bi-stable epigenetic obesity. Cell 164 , 353–364 (2015).
Michaelides, M. et al. Striatal Rgs4 regulates feeding and susceptibility to diet-induced obesity. Mol. Psychiatry . https://doi.org/10.1038/s41380-018-0120-7 (2018).
Article PubMed PubMed Central Google Scholar
Weihrauch-Blüher, S. et al. Current guidelines for obesity prevention in childhood and adolescence. Obes. Facts 11 , 263–276 (2018).
Nakamura, R. et al. Evaluating the 2014 sugar-sweetened beverage tax in Chile: An observational study in urban areas. PLOS Med. 15 , e1002596 (2018).
Colchero, M. A., Molina, M. & Guerrero-López, C. M. After Mexico implemented a tax, purchases of sugar-sweetened beverages decreased and water increased: difference by place of residence, household composition, and income level. J. Nutr. 147 , 1552–1557 (2017).
Brownell, K. D. & Warner, K. E. The perils of ignoring history: Big Tobacco played dirty and millions died. How similar is Big Food? Milbank Q. 87 , 259–294 (2009).
Mialon, M., Swinburn, B., Allender, S. & Sacks, G. ‘Maximising shareholder value’: a detailed insight into the corporate political activity of the Australian food industry. Aust. NZ J. Public Health 41 , 165–171 (2017).
Peeters, A. Obesity and the future of food policies that promote healthy diets. Nat. Rev. Endocrinol. 14 , 430–437 (2018).
Hawkes, C., Jewell, J. & Allen, K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: the NOURISHING framework. Obes. Rev. 14 (Suppl. 2), 159–168 (2013).
World Health Organisation. Global database on the Implementation of Nutrition Action (GINA). WHO https://www.who.int/nutrition/gina/en/ (2012).
Popkin, B., Monteiro, C. & Swinburn, B. Overview: Bellagio Conference on program and policy options for preventing obesity in the low- and middle-income countries. Obes. Rev. 14 (Suppl. 2), 1–8 (2013).
Download references
Reviewer information
Nature Reviews Endocrinology thanks G. Bray, A. Sharma and H. Toplak for their contribution to the peer review of this work.
Author information
Authors and affiliations.
Department of Medicine, University of Leipzig, Leipzig, Germany
Matthias Blüher
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Matthias Blüher .
Ethics declarations
Competing interests.
The author declares no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Reprints and permissions
About this article
Cite this article.
Blüher, M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol 15 , 288–298 (2019). https://doi.org/10.1038/s41574-019-0176-8
Download citation
Published : 27 February 2019
Issue Date : May 2019
DOI : https://doi.org/10.1038/s41574-019-0176-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Body composition, lifestyle, and depression: a prospective study in the uk biobank.
BMC Public Health (2024)
Physical activity, gestational weight gain in obese patients with early gestational diabetes and the perinatal outcome – a randomised–controlled trial
- Lukasz Adamczak
- Urszula Mantaj
- Ewa Wender-Ozegowska
BMC Pregnancy and Childbirth (2024)
What could be the reasons for not losing weight even after following a weight loss program?
- Jyoti Dabas
- S. Shunmukha Priya
- Praveen Budhrani
Journal of Health, Population and Nutrition (2024)
Effect of COVID-19 Pandemic Lockdowns on Body Mass Index of Primary School Children from Different Socioeconomic Backgrounds
- Ludwig Piesch
- Robert Stojan
- Till Utesch
Sports Medicine - Open (2024)
Prevalence and risk factors of obesity among undergraduate student population in Ghana: an evaluation study of body composition indices
- Christian Obirikorang
- Evans Asamoah Adu
- Lois Balmer
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

- Search Menu
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Urban Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical History
- Classical Philosophy
- Classical Mythology
- Classical Literature
- Classical Reception
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Papyrology
- Greek and Roman Epigraphy
- Greek and Roman Law
- Greek and Roman Archaeology
- Late Antiquity
- Religion in the Ancient World
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Emotions
- History of Agriculture
- History of Education
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Evolution
- Language Reference
- Language Acquisition
- Language Variation
- Language Families
- Lexicography
- Linguistic Anthropology
- Linguistic Theories
- Linguistic Typology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
- Bibliography
- Children's Literature Studies
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies (Modernism)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Media
- Music and Religion
- Music and Culture
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Science
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Lifestyle, Home, and Garden
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Politics
- Law and Society
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Neuroanaesthesia
- Clinical Neuroscience
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Toxicology
- Medical Oncology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Medical Ethics
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Security
- Computer Games
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Psychology
- Cognitive Neuroscience
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Ethics
- Business Strategy
- Business History
- Business and Technology
- Business and Government
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic History
- Economic Systems
- Economic Methodology
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Natural Disasters (Environment)
- Social Impact of Environmental Issues (Social Science)
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- International Political Economy
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Behaviour
- Political Economy
- Political Institutions
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Political Theory
- Politics and Law
- Public Policy
- Public Administration
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Developmental and Physical Disabilities Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

- < Previous chapter
26 Conclusion: Obesity and its prevention in the 21st century
- Published: September 2010
- Cite Icon Cite
- Permissions Icon Permissions
The case for a preventative approach to the obesity epidemic is compelling. Obesity poses what is arguably one of the most significant threats to population health that is currently faced. The data presented in this book highlight just how common obesity has become in children and in adults across the globe, and how it impacts disproportionately on the poor. This chapter presents a summary of the discussions in the preceding chapters.
Signed in as
Institutional accounts.
- Google Scholar Indexing
- GoogleCrawler [DO NOT DELETE]
Personal account
- Sign in with email/username & password
- Get email alerts
- Save searches
- Purchase content
- Activate your purchase/trial code
Institutional access
- Sign in with a library card Sign in with username/password Recommend to your librarian
- Institutional account management
- Get help with access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Sign in through your institution
Choose this option to get remote access when outside your institution. Shibboleth/Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Sign in with a library card
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.
Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Our books are available by subscription or purchase to libraries and institutions.
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Rights and permissions
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
How Obesity Affects Our Health Essay
Introduction, works cited.
The way the human body regulates weight is complex and interacting. There are biological, behavioral, and environmental factors included. Bodyweight is the result of how the body regulates energy intake, expenditure, and energy storage; collectively this is called energy balance (Hill 752). Obesity in terms of body mass index is 30 or more. Health risk factors begin to increase with a BMI of 25 (Schneider 272). In simpler terms, obesity is a 20% or more increase in body weight above the normal range expected as a result of fat accumulation. Obesity is a major risk factor in high blood pressure (hypertension) and certain types of diabetes (type II).
Many articles, found in the literature, explain other medical problems associated with obesity like heart disease and joint diseases (arthritis). However; the social and psychological effects of obesity received little attention (Brown 225-228). The aim of this thesis is to discuss the causal effect of obesity on hypertension, diabetes (type II), and the socio-psychological impact of obesity using a cause-effect perspective.
The association between obesity and hypertension is well documented, although the exact relationship remains unclear. Obesity activates some biochemical-hormonal mechanisms which play a role in raising blood pressure (Davy and Hall 803-813). Also, obesity is associated with increased cholesterol levels which play a role in increased blood vessels rigidity (arteriosclerosis) and accordingly hypertension. Al Atat and others (823-854) showed that control of obesity contributes to control 48% of hypertension in whites and 28% in blacks.
Studies that confirmed obesity plays a role in type II diabetes are many. Data collected by Wannamethee and Shape (1266-1272) recommend reducing the risk of type II diabetes by prevention weight gain and encouraging weight loss in obese individuals. Genuth (198-201) conducted a similar study in the UK. They suggested that most type II diabetes patients were obese or have been obese at one time in their lives. Linda and colleagues (371-377); analyzed data from the 1997-2003 National Health Interview Survey (NHIS).
They concluded that between 1997 and 2003, the incidence of diagnosed diabetes has increased among US adults. The presented data suggested that obesity is a major cause in increasing the incidence, and the incident cases of diabetes are becoming more obese.
Obesity has socio-psychological impacts on the individual (Obesity Education Initiative):
- Social unacceptability: The general impression in the US, as well as most western societies, is that; people (especially women) should be thin, and being fat is a sign of poor self-control. This creates negative attitudes about the obese that are sometimes translated into a kind of discrimination.
- Psychological disorders and obesity: Community-based studies, in the US, did not show significant differences in psychological status between obese and nonobese. In European studies, on the other hand, studies suggest an impact of obesity on emotional status.
- Overeating disorder (Binge): It means eating larger amounts of food than most people would eat in a discrete period of time (2-3 hours) with a sense of lack of control during these periods. It occurs in 20-50% of individuals who seek specialized obesity treatment.
- Body image: It is sensing one’s own body size and image and the emotional response to this image. Obese people are usually not satisfied and preoccupied with their body image and avoid social appearance. In fact, body image dissatisfaction may be a major driving cause towards treating the obesity condition.
Conclusion: Obesity is a challenging problem that needs innovative ways to tackle. Unlike smoking, where passive smokers may direct the society effort towards advertising, legislating for, and encouraging smokers not to smoke; individual eating at Mc Donald’s does not cause harm to anybody else. Therefore; the society driving force is missing. Alternatively, a great way to change eating habits is to go to public schools and start with the generations to come. Encouraging exercise (energy expenditure) is useful in health terms as well as helping those who lost weight not to regain what they lost.
Hill, James. O. Understanding and addressing the epidemic of obesity: An energy balance prospective. Endocrine Reviews. 27(7) (2006): 750-761.
Schneider, M. Introduction to Public Health (2nd ed). Pp. 225-228. Sudbury, Mass: Jones and Bartlett. 2006.
Brown, S. P. Clinical Exercise Physiology. Introduction to exercise science .. Pp. 212-234. Philadelphia, PA: Lippincott Williams & Wilkins. 2001.
Davy KP; Hall JE. Obesity and hypertension: two epidemics or one? Am J Physiol Regul Integr Comp Physiol. 286(5) (2004):R803-13.
El Atat F. Aneja A. Mcfarlane S. Sowers J. Obesity and hypertension . Endocrinol Metab Clin North Am. 32(4) (2003):823-54.
Waanamethee, S.G. and Shaper, A.G. Weight change and duration of overweight and obesity in the incidence of type 2 diabetes. Diabetes Care. 22(8) (1999): 1266-1272.
Genuth, S. Implications of the United Kingdom Prospective Diabetes Study for Patients with Obesity and Type 2 Diabetes . Obesity Research 8 (2000):198-201.
Linda, S. Geiss, M.A. Liping, P. Cadwell, B. Gregg, E.W. et al. Changes in Incidence of Diabetes in U.S. Adults, 1997–2003. American Journal of Preventive Medicine, 30(5) (2006): PP. 371-377.
Obesity Education Initiative. Clinical Guidelines on the Identification, Evaluation and Treatment of Overweight and Obesity in adults: The evidence report . National Institutes of Health. Web.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2024, March 3). How Obesity Affects Our Health. https://ivypanda.com/essays/how-obesity-affects-our-health/
"How Obesity Affects Our Health." IvyPanda , 3 Mar. 2024, ivypanda.com/essays/how-obesity-affects-our-health/.
IvyPanda . (2024) 'How Obesity Affects Our Health'. 3 March.
IvyPanda . 2024. "How Obesity Affects Our Health." March 3, 2024. https://ivypanda.com/essays/how-obesity-affects-our-health/.
1. IvyPanda . "How Obesity Affects Our Health." March 3, 2024. https://ivypanda.com/essays/how-obesity-affects-our-health/.
Bibliography
IvyPanda . "How Obesity Affects Our Health." March 3, 2024. https://ivypanda.com/essays/how-obesity-affects-our-health/.
- Sociopsychological Theories and Nursing Approaches
- Socio-Psychological Intervention for Low-Performing Students
- Socio-Psychological Trust Issues in Youth
- Socio-Psychological Factors of Abortion in Women of Different Age Groups
- Providing Age-Appropriate Care for Young Adults
- Working Conditions That Lead to Stress at Amazon
- Social Media Users' Consumer Behaviour
- Workplace Conflicts and Resolution in Nursing
- Alcohol Addiction: Opting for a Correct Referral Method
- Personality Issues Among Male People With Alcoholism
- The Rising of Obesity in America
- The Opportunity for School Food to Influence a Child’s Dietary Intake
- A Lifetime Condition – Obesity
- BMI: Assessment Tools in Adults and Children
- Obesity and Healthy Nutrition: Lesson Plan
- About Project
- Testimonials
Business Management Ideas
Essay on Obesity
List of essays on obesity, essay on obesity – short essay (essay 1 – 150 words), essay on obesity (essay 2 – 250 words), essay on obesity – written in english (essay 3 – 300 words), essay on obesity – for school students (class 5, 6, 7, 8, 9, 10, 11 and 12 standard) (essay 4 – 400 words), essay on obesity – for college students (essay 5 – 500 words), essay on obesity – with causes and treatment (essay 6 – 600 words), essay on obesity – for science students (essay 7 – 750 words), essay on obesity – long essay for medical students (essay 8 – 1000 words).
Obesity is a chronic health condition in which the body fat reaches abnormal level. Obesity occurs when we consume much more amount of food than our body really needs on a daily basis. In other words, when the intake of calories is greater than the calories we burn out, it gives rise to obesity.
Audience: The below given essays are exclusively written for school students (Class 5, 6, 7, 8, 9, 10, 11 and 12 Standard), college, science and medical students.
Introduction:
Obesity means being excessively fat. A person would be said to be obese if his or her body mass index is beyond 30. Such a person has a body fat rate that is disproportionate to his body mass.
Obesity and the Body Mass Index:
The body mass index is calculated considering the weight and height of a person. Thus, it is a scientific way of determining the appropriate weight of any person. When the body mass index of a person indicates that he or she is obese, it exposes the person to make health risk.
Stopping Obesity:
There are two major ways to get the body mass index of a person to a moderate rate. The first is to maintain a strict diet. The second is to engage in regular physical exercise. These two approaches are aimed at reducing the amount of fat in the body.
Conclusion:
Obesity can lead to sudden death, heart attack, diabetes and may unwanted illnesses. Stop it by making healthy choices.
Obesity has become a big concern for the youth of today’s generation. Obesity is defined as a medical condition in which an individual gains excessive body fat. When the Body Mass Index (BMI) of a person is over 30, he/ she is termed as obese.
Obesity can be a genetic problem or a disorder that is caused due to unhealthy lifestyle habits of a person. Physical inactivity and the environment in which an individual lives, are also the factors that leads to obesity. It is also seen that when some individuals are in stress or depression, they start cultivating unhealthy eating habits which eventually leads to obesity. Medications like steroids is yet another reason for obesity.
Obesity has several serious health issues associated with it. Some of the impacts of obesity are diabetes, increase of cholesterol level, high blood pressure, etc. Social impacts of obesity includes loss of confidence in an individual, lowering of self-esteem, etc.
The risks of obesity needs to be prevented. This can be done by adopting healthy eating habits, doing some physical exercise regularly, avoiding stress, etc. Individuals should work on weight reduction in order to avoid obesity.
Obesity is indeed a health concern and needs to be prioritized. The management of obesity revolves around healthy eating habits and physical activity. Obesity, if not controlled in its initial stage can cause many severe health issues. So it is wiser to exercise daily and maintain a healthy lifestyle rather than being the victim of obesity.
Obesity can be defined as the clinical condition where accumulation of excessive fat takes place in the adipose tissue leading to worsening of health condition. Usually, the fat is deposited around the trunk and also the waist of the body or even around the periphery.
Obesity is actually a disease that has been spreading far and wide. It is preventable and certain measures are to be taken to curb it to a greater extend. Both in the developing and developed countries, obesity has been growing far and wide affecting the young and the old equally.
The alarming increase in obesity has resulted in stimulated death rate and health issues among the people. There are several methods adopted to lose weight and they include different diet types, physical activity and certain changes in the current lifestyle. Many of the companies are into minting money with the concept of inviting people to fight obesity.
In patients associated with increased risk factor related to obesity, there are certain drug therapies and other procedures adopted to lose weight. There are certain cost effective ways introduced by several companies to enable clinic-based weight loss programs.
Obesity can lead to premature death and even cause Type 2 Diabetes Mellitus. Cardiovascular diseases have also become the part and parcel of obese people. It includes stroke, hypertension, gall bladder disease, coronary heart disease and even cancers like breast cancer, prostate cancer, endometrial cancer and colon cancer. Other less severe arising due to obesity includes osteoarthritis, gastro-esophageal reflux disease and even infertility.
Hence, serious measures are to be taken to fight against this dreadful phenomenon that is spreading its wings far and wide. Giving proper education on benefits of staying fit and mindful eating is as important as curbing this issue. Utmost importance must be given to healthy eating habits right from the small age so that they follow the same until the end of their life.
Obesity is majorly a lifestyle disease attributed to the extra accumulation of fat in the body leading to negative health effects on a person. Ironically, although prevalent at a large scale in many countries, including India, it is one of the most neglect health problems. It is more often ignored even if told by the doctor that the person is obese. Only when people start acquiring other health issues such as heart disease, blood pressure or diabetes, they start taking the problem of obesity seriously.
Obesity Statistics in India:
As per a report, India happens to figure as the third country in the world with the most obese people. This should be a troubling fact for India. However, we are yet to see concrete measures being adopted by the people to remain fit.
Causes of Obesity:
Sedentary lifestyle, alcohol, junk food, medications and some diseases such as hypothyroidism are considered as the factors which lead to obesity. Even children seem to be glued to televisions, laptops and video games which have taken away the urge for physical activities from them. Adding to this, the consumption of junk food has further aggravated the growing problem of obesity in children.
In the case of adults, most of the professions of today make use of computers which again makes people sit for long hours in one place. Also, the hectic lifestyle of today makes it difficult for people to spare time for physical activities and people usually remain stressed most of the times. All this has contributed significantly to the rise of obesity in India.
Obesity and BMI:
Body Mass Index (BMI) is the measure which allows a person to calculate how to fit he or she is. In other words, the BMI tells you if you are obese or not. BMI is calculated by dividing the weight of a person in kg with the square of his / her height in metres. The number thus obtained is called the BMI. A BMI of less than 25 is considered optimal. However, if a person has a BMI over 30 he/she is termed as obese.
What is a matter of concern is that with growing urbanisation there has been a rapid increase of obese people in India? It is of utmost importance to consider this health issue a serious threat to the future of our country as a healthy body is important for a healthy soul. We should all be mindful of what we eat and what effect it has on our body. It is our utmost duty to educate not just ourselves but others as well about this serious health hazard.
Obesity can be defined as a condition (medical) that is the accumulation of body fat to an extent that the excess fat begins to have a lot of negative effects on the health of the individual. Obesity is determined by examining the body mass index (BMI) of the person. The BMI is gotten by dividing the weight of the person in kilogram by the height of the person squared.
When the BMI of a person is more than 30, the person is classified as being obese, when the BMI falls between 25 and 30, the person is said to be overweight. In a few countries in East Asia, lower values for the BMI are used. Obesity has been proven to influence the likelihood and risk of many conditions and disease, most especially diabetes of type 2, cardiovascular diseases, sleeplessness that is obstructive, depression, osteoarthritis and some cancer types.
In most cases, obesity is caused through a combination of genetic susceptibility, a lack of or inadequate physical activity, excessive intake of food. Some cases of obesity are primarily caused by mental disorder, medications, endocrine disorders or genes. There is no medical data to support the fact that people suffering from obesity eat very little but gain a lot of weight because of slower metabolism. It has been discovered that an obese person usually expends much more energy than other people as a result of the required energy that is needed to maintain a body mass that is increased.
It is very possible to prevent obesity with a combination of personal choices and social changes. The major treatments are exercising and a change in diet. We can improve the quality of our diet by reducing our consumption of foods that are energy-dense like those that are high in sugars or fat and by trying to increase our dietary fibre intake.
We can also accompany the appropriate diet with the use of medications to help in reducing appetite and decreasing the absorption of fat. If medication, exercise and diet are not yielding any positive results, surgery or gastric balloon can also be carried out to decrease the volume of the stomach and also reduce the intestines’ length which leads to the feel of the person get full early or a reduction in the ability to get and absorb different nutrients from a food.
Obesity is the leading cause of ill-health and death all over the world that is preventable. The rate of obesity in children and adults has drastically increased. In 2015, a whopping 12 percent of adults which is about 600 million and about 100 million children all around the world were found to be obese.
It has also been discovered that women are more obese than men. A lot of government and private institutions and bodies have stated that obesity is top of the list of the most difficult and serious problems of public health that we have in the world today. In the world we live today, there is a lot of stigmatisation of obese people.
We all know how troubling the problem of obesity truly is. It is mainly a form of a medical condition wherein the body tends to accumulate excessive fat which in turn has negative repercussions on the health of an individual.
Given the current lifestyle and dietary style, it has become more common than ever. More and more people are being diagnosed with obesity. Such is its prevalence that it has been termed as an epidemic in the USA. Those who suffer from obesity are at a much higher risk of diabetes, heart diseases and even cancer.
In order to gain a deeper understanding of obesity, it is important to learn what the key causes of obesity are. In a layman term, if your calorie consumption exceeds what you burn because of daily activities and exercises, it is likely to lead to obesity. It is caused over a prolonged period of time when your calorie intake keeps exceeding the calories burned.
Here are some of the key causes which are known to be the driving factors for obesity.
If your diet tends to be rich in fat and contains massive calorie intake, you are all set to suffer from obesity.
Sedentary Lifestyle:
With most people sticking to their desk jobs and living a sedentary lifestyle, the body tends to get obese easily.
Of course, the genetic framework has a lot to do with obesity. If your parents are obese, the chance of you being obese is quite high.
The weight which women gain during their pregnancy can be very hard to shed and this is often one of the top causes of obesity.
Sleep Cycle:
If you are not getting an adequate amount of sleep, it can have an impact on the hormones which might trigger hunger signals. Overall, these linked events tend to make you obese.
Hormonal Disorder:
There are several hormonal changes which are known to be direct causes of obesity. The imbalance of the thyroid stimulating hormone, for instance, is one of the key factors when it comes to obesity.
Now that we know the key causes, let us look at the possible ways by which you can handle it.
Treatment for Obesity:
As strange as it may sound, the treatment for obesity is really simple. All you need to do is follow the right diet and back it with an adequate amount of exercise. If you can succeed in doing so, it will give you the perfect head-start into your journey of getting in shape and bidding goodbye to obesity.
There are a lot of different kinds and styles of diet plans for obesity which are available. You can choose the one which you deem fit. We recommend not opting for crash dieting as it is known to have several repercussions and can make your body terribly weak.
The key here is to stick to a balanced diet which can help you retain the essential nutrients, minerals, and, vitamins and shed the unwanted fat and carbs.
Just like the diet, there are several workout plans for obesity which are available. It is upon you to find out which of the workout plan seems to be apt for you. Choose cardio exercises and dance routines like Zumba to shed the unwanted body weight. Yoga is yet another method to get rid of obesity.
So, follow a blend of these and you will be able to deal with the trouble of obesity in no time. We believe that following these tips will help you get rid of obesity and stay in shape.
Obesity and overweight is a top health concern in the world due to the impact it has on the lives of individuals. Obesity is defined as a condition in which an individual has excessive body fat and is measured using the body mass index (BMI) such that, when an individual’s BMI is above 30, he or she is termed obese. The BMI is calculated using body weight and height and it is different for all individuals.
Obesity has been determined as a risk factor for many diseases. It results from dietary habits, genetics, and lifestyle habits including physical inactivity. Obesity can be prevented so that individuals do not end up having serious complications and health problems. Chronic illnesses like diabetes, heart diseases and relate to obesity in terms of causes and complications.
Factors Influencing Obesity:
Obesity is not only as a result of lifestyle habits as most people put it. There are other important factors that influence obesity. Genetics is one of those factors. A person could be born with genes that predispose them to obesity and they will also have difficulty in losing weight because it is an inborn factor.
The environment also influences obesity because the diet is similar in certain environs. In certain environments, like school, the food available is fast foods and the chances of getting healthy foods is very low, leading to obesity. Also, physical inactivity is an environmental factor for obesity because some places have no fields or tracks where people can jog or maybe the place is very unsafe and people rarely go out to exercise.
Mental health affects the eating habits of individuals. There is a habit of stress eating when a person is depressed and it could result in overweight or obesity if the person remains unhealthy for long period of time.
The overall health of individuals also matter. If a person is unwell and is prescribed with steroids, they may end up being obese. Steroidal medications enable weight gain as a side effect.
Complications of Obesity:
Obesity is a health concern because its complications are severe. Significant social and health problems are experienced by obese people. Socially, they will be bullied and their self-esteem will be low as they will perceive themselves as unworthy.
Chronic illnesses like diabetes results from obesity. Diabetes type 2 has been directly linked to obesity. This condition involves the increased blood sugars in the body and body cells are not responding to insulin as they should. The insulin in the body could also be inadequate due to decreased production. High blood sugar concentrations result in symptoms like frequent hunger, thirst and urination. The symptoms of complicated stages of diabetes type 2 include loss of vision, renal failure and heart failure and eventually death. The importance of having a normal BMI is the ability of the body to control blood sugars.
Another complication is the heightened blood pressures. Obesity has been defined as excessive body fat. The body fat accumulates in blood vessels making them narrow. Narrow blood vessels cause the blood pressures to rise. Increased blood pressure causes the heart to start failing in its physiological functions. Heart failure is the end result in this condition of increased blood pressures.
There is a significant increase in cholesterol in blood of people who are obese. High blood cholesterol levels causes the deposition of fats in various parts of the body and organs. Deposition of fats in the heart and blood vessels result in heart diseases. There are other conditions that result from hypercholesterolemia.
Other chronic illnesses like cancer can also arise from obesity because inflammation of body cells and tissues occurs in order to store fats in obese people. This could result in abnormal growths and alteration of cell morphology. The abnormal growths could be cancerous.
Management of Obesity:
For the people at risk of developing obesity, prevention methods can be implemented. Prevention included a healthy diet and physical activity. The diet and physical activity patterns should be regular and realizable to avoid strains that could result in complications.
Some risk factors for obesity are non-modifiable for example genetics. When a person in genetically predisposed, the lifestyle modifications may be have help.
For the individuals who are already obese, they can work on weight reduction through healthy diets and physical exercises.
In conclusion, obesity is indeed a major health concern because the health complications are very serious. Factors influencing obesity are both modifiable and non-modifiable. The management of obesity revolves around diet and physical activity and so it is important to remain fit.
In olden days, obesity used to affect only adults. However, in the present time, obesity has become a worldwide problem that hits the kids as well. Let’s find out the most prevalent causes of obesity.
Factors Causing Obesity:
Obesity can be due to genetic factors. If a person’s family has a history of obesity, chances are high that he/ she would also be affected by obesity, sooner or later in life.
The second reason is having a poor lifestyle. Now, there are a variety of factors that fall under the category of poor lifestyle. An excessive diet, i.e., eating more than you need is a definite way to attain the stage of obesity. Needless to say, the extra calories are changed into fat and cause obesity.
Junk foods, fried foods, refined foods with high fats and sugar are also responsible for causing obesity in both adults and kids. Lack of physical activity prevents the burning of extra calories, again, leading us all to the path of obesity.
But sometimes, there may also be some indirect causes of obesity. The secondary reasons could be related to our mental and psychological health. Depression, anxiety, stress, and emotional troubles are well-known factors of obesity.
Physical ailments such as hypothyroidism, ovarian cysts, and diabetes often complicate the physical condition and play a massive role in abnormal weight gain.
Moreover, certain medications, such as steroids, antidepressants, and contraceptive pills, have been seen interfering with the metabolic activities of the body. As a result, the long-term use of such drugs can cause obesity. Adding to that, regular consumption of alcohol and smoking are also connected to the condition of obesity.
Harmful Effects of Obesity:
On the surface, obesity may look like a single problem. But, in reality, it is the mother of several major health issues. Obesity simply means excessive fat depositing into our body including the arteries. The drastic consequence of such high cholesterol levels shows up in the form of heart attacks and other life-threatening cardiac troubles.
The fat deposition also hampers the elasticity of the arteries. That means obesity can cause havoc in our body by altering the blood pressure to an abnormal range. And this is just the tip of the iceberg. Obesity is known to create an endless list of problems.
In extreme cases, this disorder gives birth to acute diseases like diabetes and cancer. The weight gain due to obesity puts a lot of pressure on the bones of the body, especially of the legs. This, in turn, makes our bones weak and disturbs their smooth movement. A person suffering from obesity also has higher chances of developing infertility issues and sleep troubles.
Many obese people are seen to be struggling with breathing problems too. In the chronic form, the condition can grow into asthma. The psychological effects of obesity are another serious topic. You can say that obesity and depression form a loop. The more a person is obese, the worse is his/ her depression stage.
How to Control and Treat Obesity:
The simplest and most effective way, to begin with, is changing our diet. There are two factors to consider in the diet plan. First is what and what not to eat. Second is how much to eat.
If you really want to get rid of obesity, include more and more green vegetables in your diet. Spinach, beans, kale, broccoli, cauliflower, asparagus, etc., have enough vitamins and minerals and quite low calories. Other healthier options are mushrooms, pumpkin, beetroots, and sweet potatoes, etc.
Opt for fresh fruits, especially citrus fruits, and berries. Oranges, grapes, pomegranate, pineapple, cherries, strawberries, lime, and cranberries are good for the body. They have low sugar content and are also helpful in strengthening our immune system. Eating the whole fruits is a more preferable way in comparison to gulping the fruit juices. Fruits, when eaten whole, have more fibers and less sugar.
Consuming a big bowl of salad is also great for dealing with the obesity problem. A salad that includes fibrous foods such as carrots, radish, lettuce, tomatoes, works better at satiating the hunger pangs without the risk of weight gain.
A high protein diet of eggs, fish, lean meats, etc., is an excellent choice to get rid of obesity. Take enough of omega fatty acids. Remember to drink plenty of water. Keeping yourself hydrated is a smart way to avoid overeating. Water also helps in removing the toxins and excess fat from the body.
As much as possible, avoid fats, sugars, refined flours, and oily foods to keep the weight in control. Control your portion size. Replace the three heavy meals with small and frequent meals during the day. Snacking on sugarless smoothies, dry fruits, etc., is much recommended.
Regular exercise plays an indispensable role in tackling the obesity problem. Whenever possible, walk to the market, take stairs instead of a lift. Physical activity can be in any other form. It could be a favorite hobby like swimming, cycling, lawn tennis, or light jogging.
Meditation and yoga are quite powerful practices to drive away the stress, depression and thus, obesity. But in more serious cases, meeting a physician is the most appropriate strategy. Sometimes, the right medicines and surgical procedures are necessary to control the health condition.
Obesity is spreading like an epidemic, haunting both the adults and the kids. Although genetic factors and other physical ailments play a role, the problem is mostly caused by a reckless lifestyle.
By changing our way of living, we can surely take control of our health. In other words, it would be possible to eliminate the condition of obesity from our lives completely by leading a healthy lifestyle.
Health , Obesity
Get FREE Work-at-Home Job Leads Delivered Weekly!

Join more than 50,000 subscribers receiving regular updates! Plus, get a FREE copy of How to Make Money Blogging!
Message from Sophia!
Like this post? Don’t forget to share it!
Here are a few recommended articles for you to read next:
- Essay on Cleanliness
- Essay on Cancer
- Essay on AIDS
- Essay on Health and Fitness
No comments yet.
Leave a reply click here to cancel reply..
You must be logged in to post a comment.
Billionaires
- Donald Trump
- Warren Buffett
- Email Address
- Free Stock Photos
- Keyword Research Tools
- URL Shortener Tools
- WordPress Theme
Book Summaries
- How To Win Friends
- Rich Dad Poor Dad
- The Code of the Extraordinary Mind
- The Luck Factor
- The Millionaire Fastlane
- The ONE Thing
- Think and Grow Rich
- 100 Million Dollar Business
- Business Ideas
Digital Marketing
- Mobile Addiction
- Social Media Addiction
- Computer Addiction
- Drug Addiction
- Internet Addiction
- TV Addiction
- Healthy Habits
- Morning Rituals
- Wake up Early
- Cholesterol
- Reducing Cholesterol
- Fat Loss Diet Plan
- Reducing Hair Fall
- Sleep Apnea
- Weight Loss
Internet Marketing
- Email Marketing
Law of Attraction
- Subconscious Mind
- Vision Board
- Visualization
Law of Vibration
- Professional Life
Motivational Speakers
- Bob Proctor
- Robert Kiyosaki
- Vivek Bindra
- Inner Peace
Productivity
- Not To-do List
- Project Management Software
- Negative Energies
Relationship
- Getting Back Your Ex
Self-help 21 and 14 Days Course
Self-improvement.
- Body Language
- Complainers
- Emotional Intelligence
- Personality
Social Media
- Project Management
- Anik Singal
- Baba Ramdev
- Dwayne Johnson
- Jackie Chan
- Leonardo DiCaprio
- Narendra Modi
- Nikola Tesla
- Sachin Tendulkar
- Sandeep Maheshwari
- Shaqir Hussyin
Website Development
Wisdom post, worlds most.
- Expensive Cars
Our Portals: Gulf Canada USA Italy Gulf UK
Privacy Overview
Obesity in America: Cause and Effect Essay Sample
It is clear that the American lifestyle has contributed to the increasing prevalence of obesity. With estimates from the Washington-based Centers for Disease Prevention in the Department of Health and Human Services indicating that one in three American adults is overweight, it is evident that the country is facing an obesity epidemic. To better understand the causes and effects of obesity, research is needed to further explore the issue. For those struggling with obesity, coursework assistance may be available to help them make the necessary lifestyle changes in order to live a healthier life.
Writing a thesis paper on the topic of obesity can be extremely challenging. It requires extensive research and time to adequately cover the subject. However, there are services available that can provide assistance with the writing process. Pay for a thesis allows for the benefit of having an experienced professional provide guidance and support throughout the entire process.
Causes of Obesity
Every phenomenon must have a reason. In order to write a cause and effect essay , you need to analyze the topic carefully to cover all aspects. Obesity is considered to be a complex illness, with a number of factors contributing to its development. These can be:
- hereditary;
As you may have guessed, it is the latter category of causes and effects that we are interested in. At this point, we care about the five ones that have made the biggest contribution.
Product Range
The main cause of obesity is junk food and an unbalanced diet rich in simple carbohydrates, fats, and sugars, plus a bunch of additives. Manufactured, processed, refined, and packaged meals are the most popular. Thanks to advances in technology, Americans have come to mass-produce meals that keep fresh longer and taste better. It takes less time to prepare unhealthy, processed foods in the microwave than it does to cook them yourself.
Lack of a work-life balance, high-stress levels, insufficient sleeping hours contribute to body weight gain. Not only do these factors contribute to this, but failing to take the time to do your homework can also have a negative impact on your physical health. Without a healthy, balanced approach to work, rest, and play, you may find yourself increasingly dependent on a sedentary lifestyle that can lead to overweight consequences. Many Americans work 50, 60, or more hours a week and suffer from a deficit of leisure hours. Cooking processed foods saves them hours and money, even though they end up costing them a lot more – by causing cardiovascular disease. In addition, obese people feel stressed on a regular basis in the United States metropolitan areas. Many of them are simply binge eating under the influence of negative emotions. Chronic overeating leads to a disturbance in the appetite center in the brain, and the normal amount of food eaten can no longer suppress hunger as much as necessary, affecting the body mass.
Food Deserts
The term ‘ food desert ‘ refers to poor areas (urban, suburban and rural) with limited access to fresh fruit, grains, and vegetables – places where it is much easier to access junk food. A grocery shop in a food desert that sells healthy foods may be 10-15 miles away, while a mini-market or cheap shop that sells harmful snacks is close to the house. In such a world, it takes much more effort to eat healthier, form eating habits, and stay slim.
Everyone’s Passion for Sweets
Consuming sweets in large quantities is addictive: the more and easier we give the body energy, the more the brain uses serotonin and dopamine to encourage it – it will make obese people want sweets again and again during the day. Cakes and pastries are fast carbohydrates that easily satisfy hunger and increase body mass. Despite the harm of sweets, obese people experience the need for them to satiate. Sweetened carbonated drinks are one of the main sources of sugar in the American diet. Moreover, some individuals may be more adversely affected by such diets than others: patients with a genetic predisposition to obesity gain body mass faster from sugary drinks than those without it. This leads to childhood obesity.
The Harm of Tolerance
Every year, the body positive movement is becoming more and more popular all over the world. It would seem that this major trend should have freed us from the problems associated with the cult of thinness and society’s notorious standards. In many ways, a positive attitude towards the body has proved fruitful. For example, the notion of beauty has clearly broadened. Now on fashion shows and magazine covers, you can see not only a girl with perfectly retouched skin and without a single hint of body fat but also an ordinary person with its inherent features: overweight, wrinkles, hair, and individual skin features. In general, all the things that we are all so familiar with in real life.
Does it really make that much sense? Is this a positive thing in terms of the cause and effect topic regarding obesity? In short, opinions are divided. Extremes aren’t easy to overcome. Not everyone manages to do it. Researchers have concluded that due to plus size having become positioned as a variant of the norm, more persons have become obese. Many obese Americans have formed the opinion that it is really quite normal, and they have become oblivious to the damage it does to their health. This is what we are going to focus on next.

Effects of Obesity
We all know that obesity is dangerous to health. However, medical studies show that most adults are unaware of the number of complications and diseases that obesity in America entails. So they are fairly comfortable with becoming gradually fatter. But indifference is replaced by concern when obesity related diseases begin to occur.
For interesting examples of students writing that also reveal the causes and effects of other phenomena, consult the custom essay service offering essays by professionals. In this way, you will realize the importance of highlighting the effects right after the causes.
Is obesity an aesthetic disadvantage, an inconvenience, a limitation in physical activity or is it an illness after all? How does it affect health, and what are the consequences? The visible signs of obesity are by no means the only complication associated with this condition. Obesity creates a high risk of life-threatening diseases such as atherosclerosis, hypertension, heart attack, myocardial infarction, and kidney and liver problems. Moreover, it can also lead to disability.
Cardiovascular Disease
This is the most serious and damaging impact on the body and blood vessels in particular. Every extra kilo is a huge additional load on the heart. Obesity increases the risk of heart attacks. Experts from the American Heart Association have developed a paper on the relationship between obesity and cardiovascular disease, which discusses the impact of obesity on the diagnosis and outcomes of patients with atherosclerotic cardiovascular disease, heart failure, and arrhythmias. Childhood obesity aggravates the course of cardiovascular disease from a very early age. The fact that even kids and adolescents are obese is associated with high blood pressure, dyslipidemia, and hyperglycemia.
The result is excessive insulin production in the body. This, in turn, leads to an overabundance of insulin in the blood, which makes the peripheral tissues more resistant to it. As a consequence of the above, sodium metabolism is disturbed, and blood pressure rises. It is important to remember that excessive carbohydrate food intake leads to increased production of insulin by the pancreas. Excess insulin in the human body easily converts glucose into fat. And obesity reduces tissue sensitivity to insulin itself. This kind of vicious circle leads to type 2 diabetes.
Effects on Joints
Obesity increases the load on joints to a great extent, especially if one undergoes little or no physical activity. For instance, if one lives in a megalopolis, where all physical activity consists of getting off the sofa, walking to the car, and plumping up in an office chair at work. All this leads to a reduction in muscle mass, which is already weak, and all the load falls on the joints and ligaments.
The result is arthritis, arthrosis, and osteochondrosis. Consequently, a seemingly illogical situation is formed – there is practically no exercise, but joints are worn out harder than in the case of powerlifters. In turn, according to a study by the University of California, reducing body weight reduces the risk of osteoarthritis.
Infertility
In most cases, being obese leads to endocrine infertility, as it causes an irregular menstrual cycle. Women experience thyroid disease, polycystic ovarian syndrome, problems with conception, and decreased progesterone hormone. Obese men are faced with erectile dysfunction, reduced testosterone levels, and infertility. It should be noted that the mother’s obesity affects not only her health but also the one of her unborn child. These children are at higher risk of congenital malformations.
Corresponding Inconveniences
Public consciousness is still far from the notion that obese people are sick individuals. The social significance of the issue is that people who are severely obese find it difficult to get a job. They experience discriminatory restrictions on promotion, daily living disadvantages, restrictions on mobility, clothing choices, discomfort with adequate hygiene, and sexual dysfunction. Some of these individuals not only suffer from illness and limited mobility but also have low self-esteem, depression, and other psychological problems due to involuntary isolation by watching television or playing video games. Therefore, the public has to recognize the need to establish and implement national and childhood obesity epidemic prevention programs.
Society today provokes unintentional adult and childhood obesity among its members by encouraging the consumption of high-fat, high-calorie foods and, at the same time, by technological advances, promoting sedentary lifestyles like spending time watching television or playing video games. These social and technological factors have contributed to the rise in obesity in recent decades. Developing a responsible attitude towards health will only have a full impact if people are given the opportunity to enjoy a healthy lifestyle. At the level of the community as a whole, it is therefore important to support people in adhering to dieting recommendations through the continued implementation of evidence-based and demographic-based policies to make regular physical activity and good nutrition both affordable and feasible for all. It is recommended to cut down on the food consumed.

Related posts:
- The Great Gatsby (Analyze this Essay Online)
- Pollution Cause and Effect Essay Sample
- Essay Sample on How Can I Be a Good American
- The Power of Imaging: Why I am Passionate about Becoming a Sonographer
Improve your writing with our guides

Youth Culture Essay Prompt and Discussion

Why Should College Athletes Be Paid, Essay Sample

Reasons Why Minimum Wage Should Be Raised Essay: Benefits for Workers, Society, and The Economy
Get 15% off your first order with edusson.
Connect with a professional writer within minutes by placing your first order. No matter the subject, difficulty, academic level or document type, our writers have the skills to complete it.
100% privacy. No spam ever.

Consequences of Obesity
Health conditions, economic impact, military readiness.
People who have obesity, compared to those with a healthy weight, are at increased risk for many serious diseases and health conditions. In addition, obesity and its associated health problems have a significant economic impact on the US health care system. Obesity also affects military readiness.
Obesity in children and adults increases the risk for the following health conditions. 1,2,3
- High blood pressure and high cholesterol which are risk factors for heart disease.
- Type 2 diabetes.
- Breathing problems, such as asthma and sleep apnea.
- Joint problems such as osteoarthritis and musculoskeletal discomfort.
- Gallstones and gallbladder disease.
Childhood obesity is also associated with: 4,5,6
- Psychological problems such as anxiety and depression.
- Low self-esteem and lower self-reported quality of life.
- Social problems such as bullying and stigma.
- Obesity as adults.
Adults with obesity have higher risks for stroke, many types of cancer , premature death, and mental illness such as clinical depression and anxiety. 7,8
Annual obesity-related medical care costs in the United States, in 2019 dollars, were estimated to be nearly $173 billion. 9 Annual nationwide productivity costs of obesity-related absenteeism range between $3.38 billion ($79 per individual with obesity) and $6.38 billion ($132 per individual with obesity). 10
Direct medical costs may include preventive, diagnostic, and treatment services. Indirect costs relate to sickness and death and include lost productivity. Productivity measures include employees being absent from work for obesity-related health reasons, decreased productivity while at work, and premature death and disability 11
Just over 1 in 3 young adults aged 17-24 is too heavy to serve in the US military [PDF-774KB] . Among the young adults who meet weight requirements, only 3 in 4 report physical activity levels that prepare them for challenges in basic training. Consequently, only 2 in 5 young adults are both weight-eligible and adequately active for military service.
Also, 19% of active-duty service members had obesity in 2020, up from 16% in 2015. These individuals are less likely to be medically ready to deploy. Between 2008 and 2017, active-duty soldiers had more than 3.6 million musculoskeletal injuries. One study found that active-duty soldiers with obesity were 33% more likely to get this type of injury.
- NHLBI. 2013. Managing Overweight and Obesity in Adults: Systematic Evidence Review from the Obesity Expert Panel.
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults.
- Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5.24 million UK adults. Lancet. 2014 Aug 30;384(9945):755-65.
- Morrison KM, Shin S, Tarnopolsky M, et al. Association of depression and health related quality of life with body composition in children and youth with obesity. Journal of Affective Disorders 2015;172:18–23.
- Halfon N, Kandyce L, Slusser W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Academic Pediatrics. 2013;13.1:6–13.
- Beck AR. Psychosocial aspects of obesity. NASN Sch Nurse. 2016;31(1):23–27.
- Kasen, Stephanie, et al. “Obesity and psychopathology in women: a three decade prospective study.” International Journal of Obesity 32.3 (2008): 558-566.
- Luppino, Floriana S., et al. “Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies.” Archives of general psychiatry 67.3 (2010): 220-229.
- Ward ZJ, Bleich SN, Long MW, Gortmaker SL (2021) Association of body mass index with health care expenditures in the United States by age and sex. PLoS ONE 16(3): e0247307. https://doi.org/10.1371/journal.pone.0247307
- Trogdon JG, Finkelstein EA, Hylands T, Dellea PS, Kamal-Bahl. Indirect costs of obesity: a review of the current literature. Obes Rev .2008;9(5):489–500.
- Hammond RA, Levine R. The economic impact of obesity in the United States. Diabetes, metabolic syndrome and obesity : targets and therapy . 2010;3:285-295.
To receive email updates about this topic, enter your email address.
- Physical Activity
- Overweight & Obesity
- Healthy Weight, Nutrition, and Physical Activity
- Breastfeeding
- Micronutrient Malnutrition
- State and Local Programs
- Prevent Type 2 Diabetes
- Prevent Heart Disease
- Healthy Schools – Promoting Healthy Behaviors
- Obesity Among People with Disabilities
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HHS Author Manuscripts
Effects of Chronic Social Stress on Obesity
Karen a. scott.
Department of Psychiatry and Behavioral Neurosciences, University of Cincinnati College of Medicine, 2170 East Galbraith Road, E 212, Cincinnati, OH 45237, USA
Susan J. Melhorn
University of Washington, Harborview Medical Center, 925 Ninth Avenue, Box 359780, Seattle, WA 98104, USA
Randall R. Sakai
The prevalence of overweight and obesity has markedly increased during the past few decades. Stress has been suggested as one environmental factor that may contribute to the development of obesity. In this review, we discuss the role that exposure to chronic stress may play in the development of obesity, with particular attention to the effects of chronic psychosocial stress. Of particular importance is the effect that social stress has on dietary preference, food consumption, and regional distribution of adipose tissue. We present evidence from human and animal studies that links sympathetic nervous system and hypothalamic-pituitary-adrenal axis hyperactivity with visceral obesity, and that stress tends to alter the pattern of food consumption, and promotes craving of nutrient-dense “comfort foods.” Lastly, we discuss the visible burrow system, a model of chronic social stress used in our laboratory to assess the effects of social subordination on behavioral and metabolic profile.
Introduction
The prevalence of overweight and obesity has dramatically risen over the past few decades. Although the rate of increase has begun to slow (at least temporarily) in the United States, approximately two thirds of the population is overweight, and nearly one third is obese [ 1 ]. Initially thought to be a problem of a small number of wealthy nations, it is now clearly a global issue [ 2 ]. Although overeating and sedentary lifestyle are the most frequently cited suspects, there are likely many other contributors to the surge in obesity and obesity-related illness, including cultural, industrial, and genetic factors [ 3 , 4 ]. The “thrifty gene” hypothesis put forth by James Neel would suggest that from an evolutionary standpoint, the genetic propensity to gain weight and adiposity was adaptive —in times when food was scarce and energy demands great, it was important for the body to use nutrients efficiently and to store any excess energy for future states of negative energy balance [ 5 ]. However, John Speakman [ 6 ] hypothesizes that genes promoting obesity have always been maladaptive. He proposes that our ancestors lived in an environment that would weed out disadvantageous genes at either end of the metabolic spectrum. He notes that nearly 10% of fossilized hominids from the Pliocene era show evidence of predation [ 6 ], and that genes promoting obesity would also be selected against, as carrying excess weight would impair the ability to escape. Following the development of tools, the use of fire, and more organized social structures, humans were less vulnerable to predation. Therefore, he has proposed that this “release from predation” has allowed maladaptive genes promoting obesity to be passed down through generations in evolutionary drift [ 7 ].
Regardless of whether genes promoting obesity were ever adaptive or maladaptive, both hypotheses highlight the importance of gene × environment interactions. The disparity between the environment and lifestyle of our ancestors and that of today clearly plays a role in the development of obesity [ 5 , 8 , 9 ]. Other factors likely confer resilience or vulnerability to metabolic dysfunction. Stress has long been associated with changes in dietary preference, food intake, weight gain, and fat accrual, although specific mechanisms are less well understood. Importantly, psychological stress is linked to visceral deposition of fat, which is associated with greater health risks [ 10 – 13 ]. In this review we outline the stress response and how its derangement can negatively affect metabolic health through changes in feeding behavior and metabolic function. We review evidence from humans and animal models, with a focus on chronic social stress studies ongoing in our laboratory.
The Stress Response in Health
Stress is generally defined as a real or perceived threat to homeostasis [ 14 ]. Although often thought of as a negative thing, the stress response is critical to survival, as its function is to help the organism adapt to challenge and maintain homeostasis [ 15 ]. When one experiences acute stress (eg, a threat from a predator), the sympathetic branch of the autonomic nervous system (ANS) is rapidly activated, followed by the hypothalamic-pituitary-adrenal (HPA) axis. The ANS governs visceral functions such as respiration, heart rate, maintenance of blood pressure, hormone release, and digestion. Acute activation of the sympathetic nervous system (SNS) following stress exposure is often referred to as the “fight or flight” response. The SNS increases respiration, blood pressure, and heart rate, and activates catabolic pathways. Catecholamines bind to β-adrenergic receptors of adipocytes, inducing lipolysis via hormone-sensitive lipase. This frees nonesterified fatty acids from adipocytes and releases them into the circulation. Glycogen is hydrolyzed and gluconeogenesis is stimulated to provide glucose to tissues requiring large amounts of energy (primarily the brain, and skeletal and cardiac muscle) necessary to cope with the threat to homeostasis [ 16 ]. SNS activation inhibits the effects of insulin, and functions not necessary for immediate survival (eg, digestion, growth, and reproduction) are suppressed during this period.
Stress also triggers the HPA axis through activation of the parvocellular cells of the paraventricular nucleus of the hypothalamus (PVN). This results in the release of corticotropin-releasing hormone (CRH) and arginine vasopressin into the hypothalamo-pituitary portal circulation. CRH stimulates the synthesis and release of adrenocorticotropic hormone (ACTH) from the anterior pituitary, which binds to receptors on the adrenal cortex, inducing the release of glucocorticoids from the zona fasciculata (primarily cortisol in humans and corticosterone in rats and mice), the end product of the HPA axis [ 17 , 18 ]. Glucocorticoids bind to corticosteroid receptors, glucocorticoid (GR) and mineralocorticoid, which are, for the most part, intracellular receptors. Glucocorticoids are lipophilic and can therefore pass through cell membranes to bind with GR within the cytosol, forming a complex with other proteins. After binding, GRs translocate to the nucleus of the cell, where they act as transcription factors, binding to positive or negative glucocorticoid response elements to activate or repress gene expression. Similar to catecholamines, glucocorticoids increase lipolysis and gluconeogenesis and antagonize the anabolic actions of insulin by inhibiting both its release from pancreatic β cells, as well as its signaling abilities [ 19 ], allowing glucose, fatty acids, and amino acids to be shunted to the tissues that need them most.
In healthy individuals the stress response is short lived. Activation of the SNS is rapidly counterbalanced by the parasympathetic (“rest and digest”) branch of the ANS. The HPA response is terminated via negative feedback loops; glucocorticoids act on receptors at the level of the PVN and pituitary to inhibit the production and release of CRH and ACTH. Indirect negative feedback from limbic structures such as the medial prefrontal cortex and hippocampus also contributes to termination of the HPA axis response. Although the stress response is necessary for survival and adaptation, pathology can arise when it is prolonged. In vulnerable individuals, exposure to chronic stress can adversely affect numerous aspects of health [ 8 , 9 , 15 ].
How Can Social Stress Contribute to Obesity?
It seems counterintuitive that prolonging the stress response could result in obesity; mounting a stress response is an energetically costly activity and it serves to mobilize energy stores for immediate use. This is true for acute stress, but periods of chronic stress exposure promote acquisition and/or redistribution of energy stores. Although certainly a subjective measure, most people consider themselves “stressed,” and most frequently report that the source is social in nature. Common psychosocial stressors include low socioeconomic status, personal conflicts with friends and family, stressful work environments, lack of adequate social support, poor self-esteem, trying to balance home and work life, or caring for a sick loved one [ 8 , 20 – 22 ]. Because these are chronic types of stressors, they contribute to increased weight gain and visceral adiposity. Socioeconomic status is strongly related with disease and mortality, and has been dubbed “the status syndrome” by Marmot [ 23 ]. In the United States, poor citizens have significantly poorer health than the rich. Lack of, or inadequate, health insurance and access to health care certainly contributes to the particularly wide gap among Americans, but disparity is still observed in countries with universal health care. The gap is observed despite accounting for lifestyle differences, and Marmot [ 23 ] asserts that this is likely due to the psychological effects of low status—one’s relative status and perception of control and integration within society. Although social hierarchies are inherent in human society, the magnitude of the health disparity between the affluent and poor may be ameliorated by addressing inequalities, improving access to health care and supportive resources, providing a greater sense of control, and participation with society [ 24 ].
In addition to the metabolic effects, stress can also affect appetite and influence dietary preference. These effects are not always consistent—many people report that they tend to gain weight when they are stressed, whereas others report loss of appetite. Differences may reflect the type of stressor, its duration or severity, genetic predisposition, and learned coping style [ 25 , 26 ]. Another factor is pre-existing weight: men and women that are overweight or at the upper limits of “normal” weight are more likely to gain weight in response to stress than those that are of lower weight. It is believed that elevated insulin levels observed in heavier individuals are responsible for greater weight gain in response to stress [ 27• , 28 ]. Many people who increase food intake in response to stress report craving foods high in fats and sugar. This “comfort food” effect is thought of as non-homeostatic feeding and is proposed to activate brain reward systems and dampen stress responses. For some obese patients, overconsumption of palatable foods is thought of as a form of addiction. Imaging studies have revealed dysregulation of dopaminergic reward circuitry, similar to that observed in drug addiction [ 26 , 29• ]. Chronic social stress, access to highly palatable, energy-dense foods, and little need for physical activity set the stage for the development of overweight and obesity.
Chronic Activation of the Stress Response
Effects of chronic sympathetic activation on metabolism.
Chronic SNS activation has generally been associated with the development of obesity [ 30 – 32 ]. If SNS activation increases metabolism, mobilization of energy stores, energy expenditure, and thermogenesis, it would seem to make sense that obesity would be associated with lowered SNS activity [ 16 ]. Differences are most likely a consequence of the method by and time of assessment. Most studies agree that basal SNS activity is elevated in those with metabolic disorders. However, there is some disagreement about what happens in response to challenge, such as insulin administration or cold stress [ 16 , 33 ]. Studies suggest that although basal SNS activity may be chronically elevated, the response to stress is blunted. It is hypothesized that these high levels of basal catecholamines induce downregulation or desensitization of adrenergic receptors in adipose tissue. This, in turn, inhibits lipolysis upon activation of the SNS, and leads to insulin resistance. Spraul et al. [ 31 ] found that increased SNS activity, as measured by muscle sympathetic nerve activity, was directly related to body composition. Others have demonstrated that men with low job status have lower heart rate variability, indicating enhanced sympathetic activity [ 34 ]. But is SNS hyperactivity a cause or consequence of obesity? Recent studies have indicated that heightened sympathetic activity may precede overweight and obesity in individuals. Elevated resting and ambulatory heart rate have been directly related to overweight and obesity in follow-up examinations of hypertensive patients [ 35 ]. Similarly, a prospective study of healthy, nonobese males found that those with elevated plasma norepinephrine gained more weight over a 5-year period [ 36 ].
HPA Axis Hyperactivity
Chronic activation of the HPA axis has been associated with numerous pathologies, including metabolic disorders. In fact, many of the symptoms of the metabolic syndrome are shared with those of Cushing’s syndrome, caused by hypercortisolism. These include the preferential deposition of adipose tissue in the midsection, hypertension, dyslipidemia, and insulin resistance [ 37 – 39 ]. Although an acute stress response promotes mobilization of energy stores for use, chronic glucocorticoid exposure has the opposite effect, promoting energy storage as fat, and preferentially within the abdomen. For example, chronic variable stress or administration of exogenous corticosterone increases body weight, mesenteric fat pad weight, leptin levels, and adipocyte size of rodents [ 13 , 40 ]. The overall effects of glucocorticoid exposure differ by tissue type. Chronic glucocorticoid exposure increases the expression and activity of lipoprotein lipase within adipose tissue depots, facilitating fat storage, and this predominates within visceral adipose tissue since visceral depots express more GR than subcutaneous depots. The stromal vascular cells of visceral adipose express higher levels of 11β-hydroxysteroid dehydrogenase (11β-HSD-1), an enzyme that regenerates glucocorticoids from their inactive metabolites, further augmenting local glucocorticoid action in abdominal fat [ 41 , 42 ].
Does Social Stress Cause Human Obesity?
Numerous epidemiologic studies have linked social stress with obesity and metabolic disorders. However, it is difficult to determine whether stress contributes to the development of metabolic dysfunction or is a result of metabolic dysfunction itself. Because of the difficulties associated with long-term studies, many rely on measures taken over a short period of time, metabolic response to acute stressors, or retrospective studies. However, some recent studies have looked at psychosocial factors and metabolic function over longer periods of time. Beginning with baseline measures taken in the mid- to late 1980s, health data have been regularly collected from a large group of UK civil servants, in what is referred to as the Whitehall II Studies. One recent follow-up found that men and women who reported long-term conflicts within, or lack of support from, their closest relationships were more likely to have had an increase in waist circumference and body mass index (BMI) over the study period [ 43 ]. Others studying the Whitehall II cohort have found associations between chronic stress and other factors associated with metabolic syndrome, such as elevated basal sympathetic activity or prolonged sympathetic response to stress [ 21 , 34 ]. Similarly, a recent Finnish study conducted over a 6-year period found that adults self-reporting psychological distress had a significantly higher likelihood of developing the metabolic syndrome by study end [ 44 ].
A particularly troubling issue is the number of children and adolescents who are classified as overweight or obese. Recent estimates indicate that approximately 17% of children in the United States are obese [ 45 ]. It is already well established that childhood obesity often persists into adulthood, and recent studies suggest that childhood overweight and obesity are associated not only with poor health in adulthood, but shortened lifespan [ 46 ]. As in adults, the nutritional and social environment likely plays a large role in pediatric obesity. Although we are all exposed to social stressors, adolescents may be particularly vulnerable to their deleterious effects on health [ 47 ]. Adolescence is a period of development associated with the desire for more independence from family, which can lead to conflict. Desire for acceptance from peers can lead to significant social pressure. It is also a period in which the brain is still developing and attitudes about food and coping behaviors are learned. Although the overall rise in childhood obesity has slowed, it has not for those from disadvantaged backgrounds [ 48 ]. Low income has been associated with higher risk of childhood overweight and obesity in several studies [ 47 , 49 – 52 ]. Stamatakis et al. [ 53•• ] contend that there is in fact a growing divide between the upper class and those with a lower socioeconomic status.
Animal Models of Stress
Because of obvious technical and ethical constraints, there are limitations to stress studies in humans. Clearly, it is not ethical to purposefully subject humans to chronic social stress. It takes decades to conduct prospective studies of long-term social stress on human health. For these reasons, animal models can help to elucidate mechanisms by which stress impacts physiology. It is of great importance to thoughtfully consider the model that is used; it should be ethologically relevant to the animal, and should also translate to the human condition. Although in the past it was assumed that all stressors were generally the same, we now realize that psychological and physiologic stressors can utilize very different neural circuitry [ 54 , 55 ]. Therefore, studies of social species in a social environment may be most useful in modeling the human condition. Numerous species have been used to study stress effects, including nonhuman primates, rodents, and zebrafish.
Nonhuman primates have provided invaluable insight into the effects of social stress; since they are most closely related to humans, they share many physiologic and neuroanatomical features. Female nonhuman primates have a reproductive cycle that more closely resembles that of humans, and many nonhuman primate species also form dominance hierarchies, allowing for the investigation of sexually dimorphic effects of social subordination. Nonhuman primates also share many of the same genetic polymorphisms as humans that have been associated with vulnerability or resilience to disease. Their average lifespan is considerably shorter than humans, but much longer than those of rodents, which makes them ideal for longitudinal studies. Although less closely related to humans than nonhuman primates, rats and mice still share many similarities, which are supported by a rich literature of behavior and comparative anatomy and physiology. Because of their size and shorter lifespan, they require far fewer resources (time, space, and economic) and can provide valuable information over a shorter period of time than nonhuman primates. A particular strength of rodent models is the wide variety of strains available. Rats and mice have been selectively bred for particular traits such as coping style, susceptibility to disease, and diet-induced obesity [ 56 – 58 , 59• , 60 ]. Additionally, the ability to look at the effects of down- or upregulation of gene expression via spontaneous mutations, transgenics, and the use of viral vectors yields invaluable information on genetic vulnerability or resilience to disease [ 61 – 65 ]. Zebrafish (Danio rerio) may also help us to elucidate the genetic and epigenetic mechanisms that underpin behavioral or coping strategies. These social fish have a well-documented behavioral repertoire and share similar neuroendocrine and neurotransmitter systems and basic neuroanatomy to those in humans, nonhuman primates, and rodents. A particular strength of the zebrafish is that its genome has been fully sequenced, and a number of mutant models are available for study [ 66 ]. For instance, zebrafish with a mutation of the fibroblast growth factor receptor 1a ( fgfr1a ) gene engage in more exploration of a novel environment, spend more time in proximity to a novel object, and exhibit more aggressive behaviors toward a “conspecific” (reaction to its own reflection in a mirror). This single mutation appears to influence the temperament or coping style of the zebrafish [ 67 ]. It appears that the gene affects behavior through its influence on histamine expression, which is reduced in the fgfr1a mutant fish. Restoring histamine to normal levels resulted in behavior similar to that of wild-type zebrafish. It is also possible to study the effects of social stress in zebrafish, as dominance is established when males are pair-housed [ 68 ].
Social stress in animals affects food intake, food preference, and body composition. Subordinate (SUB) nonhuman primates exhibit behavioral and physiologic symptoms of stress, including depressive-like behaviors and increased HPA axis and SNS activity. Sexually dimorphic effects on fat deposition exist in both humans and nonhuman primates, and can therefore facilitate study into the mechanisms by which males are more vulnerable to developing visceral obesity. In male cynomolgus macaques, social instability (generated by frequently changing the composition of social groups) results in increased coronary artery atherosclerosis and deposition of abdominal adipose tissue [ 69 , 70 ]. Males with the greatest heart rate responses to stressors (a measure of sympathetic activation) also have the most severe atherosclerosis [ 69 ]. SUB female rhesus macaques consume more calories than dominant (DOM) females when provided with a standard diet. When provided with a choice between the standard diet and a highly palatable high-calorie diet, both DOM and SUB females preferred the high-calorie diet, but the SUB females continue to consume more than the DOM females. When provided with a moderate-fat diet, SUB female cynomolgus monkeys are more likely to centralize fat stores than DOM females [ 71 , 72 ]. Similarly, SUB male mice consume more high-fat diet than DOM males, and have improved caloric efficiency, leading to weight gain and elevated plasma glucose and free fatty acids.
Access to and consumption of palatable food and drink appears to ameliorate or prevent some of the behavioral and physiologic effects of stress. In the previously mentioned study, consumption of the high-calorie diet was associated with a decrease in aggression and anxiety-related behaviors in SUB female cynomolgus monkeys [ 73 ]. Male rats provided daily access to a small amount of sweetened solution have a blunted HPA axis response to acute stressors such as restraint [ 74 , 75• ].
The Visible Burrow System
Our laboratory examines the effects of chronic social stress on metabolism using the visible burrow system (VBS), which is used to create a semi-natural, ethologically relevant habitat for socially housed rats. It consists of a series of tunnels and chambers, meant to simulate burrows formed by wild rats, and an open surface area exposed to a 12:12 light cycle ( Fig. 1 ). When males and females are housed within this system, males form a dominance hierarchy. SUB males exhibit signs of social stress including lower testosterone, elevated corticosterone, adrenal hypertrophy, thymic involution, hypophagia, and weight loss over the 2-week housing period [ 76 – 79 ]. At the end of this period, both DOM and SUB males lose fat mass, but SUB males lose a greater proportion of subcutaneous to visceral adipose tissue than DOM males. SUB males also lose a significant amount of lean tissue. Upon removal and a 3-week recovery period of single housing, SUB males are hyperphagic and accrue a significant amount of adipose tissue, preferentially stored in visceral depots [ 77 , 80 , 81 ]. This suggests increased visceral adiposity, despite the finding that the body weight does not return to that of DOMs and CONs (controls; singly housed males) during a 3-week recovery period. This is similar to a recent cross-sectional study of men that found that although self-reported stress scores did not correlate with BMI, they were directly related to body composition [ 82 ]. In the VBS, body compositional effects are enhanced by multiple cycles through VBS and recovery [ 81 , 83• ]. On the surface, the VBS model differs from animal and human models in that the most socially stressed animals lose weight. However, this may be an effect of the severity of the social stress within the burrow. The release and recovery from this stress is likely responsible for the rapid recovery of weight and preferential deposition of visceral fat. When SUBs come out of the VBS, they have elevated glucocorticoids, low testosterone, and upregulation of orexigenic hypothalamic neuropeptides, which most likely contributes to this phenotype. Much of our recent research has focused on the mechanisms by which this preferential fat gain occurs. Two recent studies have focused on the roles of pattern of food ingestion and nutrient trafficking during and following subordination stress.

Illustrates the visible burrow system with food intake monitoring equipment
Stress-Induced Changes in Feeding Behavior
One area of interest is how feeding patterns are altered during VBS housing and recovery. Others have demonstrated that the manner in which one consumes food can affect weight gained and/or body composition, even when the total caloric intake is the same [ 84 – 86 ]. Monitoring food intake of group housed animals is not an easy task; continuous video recording allowed us to determine when each rat was at a feeder, but it was not suitable for studying how much food was consumed or the microstructure of meals. In collaboration with AccuScan Instruments (Columbus, OH) and the University of Cincinnati (UC) Biomedical Engineering Department, we have modified a meal pattern system (Dietmax ID, AccuScan Instruments) with which to study the meal patterns of males within the VBS ( Fig. 1 ). Prior to the study, each male is implanted with a small microchip that can be read by scanners located above feeding cups within the VBS. The food cups sit upon scales connected to an analyzer which records, with a timestamp, all changes in cup weight (Dietmax ID System). This allows us to determine where and when each rat fed, in addition to the amount of food consumed. The UC Biomedical Engineering Department has developed a program in which these data can be analyzed to determine meal patterns for each animal; the number of meals taken, size of individual meals, duration of meals, and intermeal interval, a measure of time taken between meals. A more thorough explanation of the meal pattern equipment can be found in a recently published study by Melhorn et al. [ 83• ]. The food intake of DOMs and SUBs decreases significantly during the first day of VBS housing, as the dominance hierarchy is established. However, DOMs rapidly return to their basal food intakes. The reduction in food intake of SUBs persists through the duration of VBS housing, and occurs through a reduction in both the size and number of meals. This reduction occurs voluntarily; food is readily available in each chamber and the open surface area. The temporal pattern of food intake of SUBs is markedly altered. Whereas DOMs and CONs consume the bulk of their meals during the dark period (since rats are a nocturnal species), SUBs take meals throughout the 24-hour period, including many during the light period [ 83• ].
When SUBs are removed from the VBS and allowed to recover in individual cages, they are hypercorticosteronemic and hyperphagic. SUBs consume fewer meals, but the meal size is significantly greater than CONs, a pattern associated with preferential adipose gain, as noted previously. They also continue to consume more meals during the light period during the first week of recovery, which may further contribute to weight gain during recovery, as disrupted sleep or reverse feeding represent additional stressors associated with sympathoadrenal hyperactivity–altered metabolic profile and obesity [ 40 , 87 , 88 ]. Although DOMs regain adipose tissue during a 3-week recovery period, SUBs have a much more exaggerated gain in adiposity, which is most pronounced during the first week of recovery [ 83• ].
Stress-Induced Changes in Glucose Trafficking
Glucose trafficking may play an important role in body composition changes during and in recovery from social stress. Epidemiologic studies have found that psychosocial stressors correlate to poor glycemic control [ 82 , 89 ]. We have recently begun to examine the effects of social stress on glucose transporter 4 (GLUT4) expression of SUB rats during VBS housing and following a recovery period. GLUT4 is an insulin-dependent glucose transporter located in adipose tissue, muscle, and brain. Insulin stimulates translocation of GLUT4 from vesicles within the cytosol to the plasma membrane, and enabling glucose uptake into the cell. Chronic activation of the stress response is associated with insulin resistance, impairing GLUT4-mediated glucose uptake. GLUT4 expression is highly regulated by glucocorticoids and transcription can be directly modulated by local glucocorticoid levels. Our preliminary data indicate that DOM males have an increased ratio of plasma membrane (translocated, active) to whole membrane (cytosolic) GLUT4 protein in skeletal muscle, compared with CONs and SUBs, suggesting a mechanism by which DOMs preferentially gain lean tissue in recovery. We find that SUBs are not glucose intolerant at the end of VBS housing, despite elevated corticosterone levels. This is most likely due to increased physical activity within the burrow, which has been shown to increase muscle GLUT4 translocation and insulin sensitivity; offsetting the suppressive effects of elevated glucocorticoids [ 90 ]. We are currently looking at GLUT4 expression in different adipose depots of DOMs, CONs, and SUBs. Although many studies report that elevations in glucocorticoids inhibit insulin sensitivity in both adipose tissue and skeletal muscle, others have found that elevations can enhance insulin sensitivity in human adipocytes [ 91 ]. Increased adipose gain in SUBs during recovery suggests that there may be an upregulation in adipose GLUT4 expression, or an enhancement of translocation from intracellular stores to the plasma membrane, augmenting glucose uptake.
Conclusions
Obesity and its associated health risks have risen dramatically in the past few decades. Sedentary lifestyle and easy accessibility to highly palatable nutrient-dense foods creates an environment that promotes overweight and obesity. Chronic social stress, often arising from poor interpersonal relationships, job or unemployment stress, poor self-esteem, and low socioeconomic status has been associated with obesity and its associated illnesses. Chronic activation of the SNS and HPA axis contribute to a anabolic state that promotes fat storage within visceral depots, which increases the risk of dyslipidemia, type 2 diabetes, cardiovascular disease, and other facets of the metabolic syndrome. Stress can also enhance weight gain and fat deposition through changes in feeding behavior. Chronic stress is known to alter the pattern of food intake, dietary preference, and the rewarding properties of foods.
Animal models, such as colony housing of rodents and nonhuman primates have provided invaluable insight into the mechanisms by which obesity may arise from social stress exposure. Although the ideal model to study effects of stress on humans is, of course, humans, ethical and logistical issues often preclude such studies. Human responses to social stress also vary widely among individuals, and it is impossible to completely control for aspects of individual personal experience. For these reasons, ethologically relevant animal models of social stress can fill an important void in understanding how social stress may contribute to obesity.
Of course, there are some aspects that cannot be modeled in animals. Some emotions experienced in response to social stress such as shame, guilt, and self-consciousness are considered by most to be unique to humans. Therefore, it is important to consider animal studies as a complement to studies in humans that may provide insight into the neural mechanisms and genetic factors that underlie stress-associated illness. This in turn may facilitate the development of interventions that may prevent and/or treat stress-related metabolic dysfunction.
Disclosure Conflicts of interest: K.A. Scott: is supported by National Institutes of Health (NIH) grant MH088230; S.J. Melhorn: none; R.R. Sakai: has been a board member for Physiology & Behavior ; has been a grant reviewer for the National Science Foundation; is employed by the University of Cincinnati; is supported by NIH grant DK068273, and a grant from the Department of Defense; and has received travel/accommodations expenses covered or reimbursed from the National Science Foundation.
Contributor Information
Karen A. Scott, Department of Psychiatry and Behavioral Neurosciences, University of Cincinnati College of Medicine, 2170 East Galbraith Road, E 212, Cincinnati, OH 45237, USA.
Susan J. Melhorn, University of Washington, Harborview Medical Center, 925 Ninth Avenue, Box 359780, Seattle, WA 98104, USA.
Randall R. Sakai, Department of Psychiatry and Behavioral Neurosciences, University of Cincinnati College of Medicine, 2170 East Galbraith Road, E 212, Cincinnati, OH 45237, USA.
Papers of particular interest, published recently, have been highlighted as:
• Of importance
• • Of major importance
IMAGES
VIDEO
COMMENTS
Moreover, obesity causes diabetes, especially among adults as the body may become resistant to insulin. This resistance may lead to a high level of blood sugar, which is fatal. Besides health complications, obesity causes an array of psychological effects, including inferiority complex among victims. Obese people suffer from depression ...
Obesity has become a global epidemic and is one of today's most public health problems worldwide. Obesity poses a major risk for a variety of serious diseases including diabetes mellitus, non-alcoholic liver disease (NAFLD), cardiovascular disease, hypertension and stroke, and certain forms of cancer (Bluher, 2019).Obesity is mainly caused by imbalanced energy intake and expenditure due to a ...
This essay will explore the various causes of obesity and their effects on individuals and society as a whole. One of the primary causes of obesity is dietary habits and nutritional intake. The consumption of high-calorie, low-nutrient foods, such as fast food, sugary beverages, and processed snacks, has become increasingly prevalent in modern ...
Introduction. Obesity is an increasing, global public health issue. Patients with obesity are at major risk for developing a range of comorbid conditions, including cardiovascular disease (CVD), gastrointestinal disorders, type 2 diabetes (T2D), joint and muscular disorders, respiratory problems, and psychological issues, which may significantly affect their daily lives as well as increasing ...
Despite public health efforts, these disorders are on the rise, and their consequences are burgeoning. 1 The Centers for Disease Control and Prevention report that during 2017 to 2018, the prevalence of obesity in the United States was 42.4%, which was increased from the prevalence of 30.5% during 1999 to 2002. 2 Among those afflicted with ...
1. Introduction. Obesity is a complex, multifactorial, and largely preventable disease (), affecting, along with overweight, over a third of the world's population today (2,3).If secular trends continue, by 2030 an estimated 38% of the world's adult population will be overweight and another 20% will be obese ().In the USA, the most dire projections based on earlier secular trends point to ...
Obesity and Diabetes. The condition most strongly influenced by body weight is type 2 diabetes. In the Nurses' Health Study, which followed 114,000 middle-age women for 14 years, the risk of developing diabetes was 93 times higher among women who had a body mass index (BMI) of 35 or higher at the start of the study, compared with women with BMIs lower than 22.
Obesity is a disease with a major negative impact on human health. However, people with obesity may not perceive their weight to be a significant problem and less than half of patients with obesity are advised by their physicians to lose weight. ... A meta-analysis of MR studies confirms the causal effect of obesity on NAFLD, with central ...
Obesity prevalence among children is >30% in the Cook Islands, Nauru and Palau, with a notable increase over the past few decades. Worldwide prevalence of obesity increased at an alarming rate in ...
Over this same 50-year period, the scientific evidence regarding the effects of obesity on health and well-being has also grown. The immediate and long-term physical and psychosocial health effects of obesity on individuals, both direct and indirect, are substantial, and experienced by children as well as adults, as illustrated in Chapters 3-5 .
Obesity in terms of body mass index is 30 or more. Health risk factors begin to increase with a BMI of 25 (Schneider 272). In simpler terms, obesity is a 20% or more increase in body weight above the normal range expected as a result of fat accumulation. Obesity is a major risk factor in high blood pressure (hypertension) and certain types of ...
Obesity is a growing concern in many parts of the world, with rates on the rise. According to the World Health Organization (WHO), obesity has more than doubled globally since 1980. This essay will examine the causes of obesity, including dietary habits, sedentary lifestyles, and genetic factors, and explore the significant effects it has on individuals and society as a whole.
Essay on Obesity - For College Students (Essay 5 - 500 Words) Obesity can be defined as a condition (medical) that is the accumulation of body fat to an extent that the excess fat begins to have a lot of negative effects on the health of the individual.
People who have overweight or obesity*, compared to those with healthy weight, are at increased risk for many serious diseases and health conditions. These include: 1,2,3. All-causes of death (mortality). High blood pressure (hypertension). High LDL cholesterol, low HDL cholesterol, or high levels of triglycerides (dyslipidemia). Type 2 diabetes.
The main cause of obesity is junk food and an unbalanced diet rich in simple carbohydrates, fats, and sugars, plus a bunch of additives. Manufactured, processed, refined, and packaged meals are the most popular. Thanks to advances in technology, Americans have come to mass-produce meals that keep fresh longer and taste better.
Effects of obesity. Obesity has serious health consequences such as type 2 diabetes, cardiovascular disease, stroke, and some types of cancer. These conditions are associated with high morbidity and mortality rates. Obesity can also cause respiratory problems, sleep apnea, and osteoarthritis.
Joint problems such as osteoarthritis and musculoskeletal discomfort. Gallstones and gallbladder disease. Childhood obesity is also associated with: 4,5,6. Psychological problems such as anxiety and depression. Low self-esteem and lower self-reported quality of life. Social problems such as bullying and stigma.
In this essay I will be addressing why obesity is an important subject within health and wellbeing at present. Obesity still affects around one in four people that are adults and one in every 5 children around the ages of ten to eleven years old that live within the United Kingdom. ... There's also a mental effect of obesity as it can affects ...
Accordingly, 93 papers are identified from the review articles as primary studies from an initial pool of over 700 papers addressing obesity. Consequently, this study initially recognized the significant potential factors that influence and cause adult obesity. ... To investigate major diseases, conditions, and other negative health effects ...
This is a free essay sample available for all students. If you are looking where to buy pre written essays on the topic "Cause and Effects of Obesity", browse our private essay samples.. Many people don't know this but obesity is not just a body cosmetic condition it's a complex disease. According to CDC (Centers for Disease Control and Prevention), obesity is diagnosed when a person ...
Endotoxin is a general term for toxic substances in Gram-negative bacteria, whose damaging effects are mainly derived from the lipopolysaccharides (LPS) in the cell walls of Gram-negative bacteria, and is a strong pyrogen. Obesity is a chronic, low-grade inflammatory condition, and LPS are thought to trigger and exacerbate it. The gut flora is the largest source of LPS in the body, and it is ...
Introduction. The prevalence of overweight and obesity has dramatically risen over the past few decades. Although the rate of increase has begun to slow (at least temporarily) in the United States, approximately two thirds of the population is overweight, and nearly one third is obese [].Initially thought to be a problem of a small number of wealthy nations, it is now clearly a global issue [].
In addition, its effects are positive against visceral obesity, a particularly worrying fat that accumulates deep in the abdomen, close to vital organs, which can cause serious health problems.
The Pfizer and Moderna COVID-19 vaccines can cause myocarditis, but do not appear to cause infertility, Guillain-Barré syndrome, Bell's palsy, thrombosis with thrombocytopenia syndrome (TTS) or heart attack, according to a new National Academies of Sciences, Engineering, and Medicine report examining whether COVID-19 vaccines can cause certain harms.